
Abstract
In 2023, passive laboratory-based surveillance showed an increase in hepatitis A virus (HAV) infection. We investigated hepatitis A incidence using the notifiable medical condition surveillance system (NMCSS) data and molecularly characterised positive blood samples from the Western Cape province for 2023. All HAV IgM seropositive cases from the NMCSS from 1 January to 31 October 2023 in South Africa were investigated. HAV RNA from blood samples that had tested positive for HAV IgM from Western Cape was amplified in the VP1/P2B junction and sequenced (3500Xl Genetic Analyser). Sequences were assembled, aligned (Sequencher) and analysed (Aliview 1.27 and MEGA11). Statistical analysis was performed using Excel and the CuSum2 Threshold to determine suspected outbreaks. In 2023, the incidence of HAV IgM was 6.28/100,000 in South Africa, with the highest incidence in Western Cape province (15.86/100,000). Children aged 5 to 14 years were affected the most in the Western Cape. The positive cases in the Western Cape were above the CuSum2 threshold from January to May 2023, with the highest incidence observed in the City of Cape Town Metropolitan (14.8/100,000). Genotyping was successfully performed on 92.7% (139/150) of serum samples, for which the IB sub-genotype was detected. Three primary mutations R63K, R71S and M104I were observed in more than 49% of the samples. Most of the samples sequenced belonged to patients residing in areas close to each other within the City of Cape Town Southern, Western, and Mitchells Plain sub-districts. The CuSum2 threshold method allowed the identification of suspected HAV outbreaks in the districts within the Western Cape in 2023 while genotyping identified clusters of sub-genotype IB. Genotyping could assist with determining the common source of infection during an outbreak, especially if coupled with epidemiological and geographical data. Further active surveillance can assist in investigating the HAV risk factors for targeted public health responses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatitis A virus (HAV) is one of the viral aetiological agents responsible for causing acute liver disease and cirrhosis [1]. The virus is hyper-endemic in sub-Saharan Africa and South Asia [2]. Transmission occurs through the faecal-oral routes between infected individuals or contaminated food or water sources and can be detected in blood or stool [3]. Low to middle income countries are usually at higher risk of transmitting HAV within the population due to poor hygiene and sanitary conditions [1]. Symptomatic individuals can commonly present with jaundice, fever, dark urine, malaise, nausea and abdominal discomfort, that may last less than 2 months [1, 3]. Symptomatic presentation among HAV infected individuals is directly linked to age. Approximately 70% of children below 6 years of age are either asymptomatic or if they are symptomatic, may not be affected by jaundice [3, 4]. In contrast, older children and adults are commonly symptomatic and present with jaundice [3].
In South Africa, HAV infection is a notifiable medical condition (NMC) and considered highly endemic, as it is assumed most children are exposed by 6 years of age [5]. From 2005 to 2015, the HAV seroprevalence rates in the public health sector were described and anti-HAV IgM was reported in 3.3% (16 423/ 501 083) of individuals, of which an estimated 34% were among children 1–4 years of age and < 0.5% were adults older than 45 years [4]. In the Western Cape province, a surveillance study from 2009 to 2014 based on acute hepatitis A cases from the National Institute for Communicable Diseases (NICD), showed HAV IgG positivity was pronounced at 6 years of age with < 90% seropositivity by the age of 10 years achieved from 2009 [6]. In the Gauteng province, an HAV IgG and IgM seroprevalence study from 2018 to 2019, on HIV-infected and -uninfected children, reported < 90% seropositivity by the age of 10 years (68.6%), similar to the previous study described, which was an indication of an intermediate endemicity [7]. The latter study confirmed older individuals and informal settlements are linked to an increase in HAV seropositivity. From 2017 to 2020, the HAV incidence in KwaZulu-Natal, Gauteng and Western Cape provinces were highest among children aged < 5 to 9 years of age and an outbreak was detected in Overberg district in the Western Cape [8]. Overall in South Africa, NMC surveillance system (NMCSS) reported 1 538 HAV infections in 2022, with 35% of cases belonging to children < 10 years of age. The incidence of HAV was 3 per 100 000 in South Africa in 2022, with the Western Cape having the highest incidence at 7 per 100 000 and the remaining provinces an incidence of 3 per 100 000 [5]. Hepatitis A is shown to transitioning to intermediate endemicity in Western Cape province and South Africa [6, 7]. In South Africa, the hepatitis A vaccine is not part of the expanded program on immunization (EPI) although it is available in the private sector for children at 12 and 18 months of age [8].
HAV is a non-enveloped RNA virus, belonging to the genus Hepatovirus within the Picornaviridae family [3, 9]. HAV is classified into 6 genotypes (I to VI) based on the genomic characterisation of the VP1 region, but only has a single serotype [10, 11]. Genotypes I to III infect humans and genotypes IV to VI circulate among simians. The genotypes are further classified into sub-genotypes A and B [10]. Genotype I was detected globally with IA being most prevalent in Europe, Asia, North and South America, and Africa [11, 12]. Sub-genotypes IA and IB commonly co-circulate in several regions globally [10]. IA is most prevalent in South and North Americas, Europe, Asia and Africa. Genotype IB is predominantly observed in the Middle East, South Africa and some parts of South America [11,12,13]. Genotype II originated from West Africa but is not commonly detected. Genotype III also circulates globally, with IIIA dominant in Korea, Russia and Europe [10]. The clinical significance of the different genotypes is still unknown. HAV is genetically heterogeneous in various parts of the genome which is a trait widely used to investigate the genetic relatedness of HAV strains circulating in a community during an outbreak investigation. The Centers for Disease, Control and Prevention (CDC) showed that the HAV genotypes can be accurately detected by sequencing the VP1-P2B region, including highly variable P2A region, when compared to the VP1 region [3].
Previously, a passive laboratory-based surveillance approach was successfully implemented to analyse hepatitis A cases notified through the NMCSS [8]. NMCSS offers accurate analysis and epidemiological reporting informed by the public and private healthcare sectors which allows for a rapid public health response. In this study, we used the NMCSS with the addition of geographic location and genotypic characterisation to describe the incidence of HAV and investigate further the positive cases from the Western Cape province in South Africa for the period from January to October 2023.
Methods
Study population and specimen collection
All HAV IgM positive cases recorded in the Surveillance Database Warehouse (SDW) and reported on the NMCSS from 1 January to 31 October 2023 from all nine provinces of South Africa were included in this study. Data was de-duplicated by removing duplicate folder numbers and patient unique IDs. All participants’ data was anonymised in an aggregated form.
For laboratory investigation, patients who tested positive for HAV IgM, at the National Health Laboratory Services (NHLS) in Groote Schuur hospital, Western Cape province, South Africa, from 12 March to 07 October 2023, were included for genotyping. After testing for IgM, the residual serum samples were received at the (NICD), Centre for Vaccines and Immunology, for genotyping. Patient data was merged with the NMCSS data through the SDW. All participants’ data was anonymised in an aggregated form by assigning a unique laboratory ID to each patient sample.
Statistical analysis
Demographic data analysed included age groups, gender, district and sub-districts of individuals with HAV from the Western Cape. The CuSum2 threshold was determined for the period from 2019 to 2023, as previously described [8], which displays a threshold based on the mean + 3SD for each rolling 7-month period (excluding the two most recent points) as an action level.
Genotyping using Sanger sequencing
Extraction
RNA was extracted using the QiAmp RNA extraction kit (Qiagen, Germany), following the manufacturer’s instructions with a double elution of 40 µl each.
Amplification
The RNA was subjected to cDNA synthesis using SuperScript IV reverse transcription kit (Invitrogen, United States) with random hexamers, as per manufacturer’s instructions. Nested PCR was performed using HotStarTaq Master Mix (Qiagen, Germany) and amplifying the VP1-P2B junction. The first round PCR was performed using 10µM 2870P forward primer (GACAGATTCTACATTTGGATTGGT) and 10µM 3381 N reverse primer (CCATTTCAAGAGTCCACACACT), previously described [14]. The cycling conditions were as follows: activation at 95 °C for 15 min, with 35 cycles of denaturation at 94 °C for 30 s, annealing at 50 °C for 48 s, and extension at 72 °C for 1 min, with a final extension at 72 °C for 10 min. The second round PCR was performed using 5 µl of the first round PCR product with 10µM 2896P forward primer (CTATTCAGATTGCAAATACAAT) and 10µM 3289 N reverse primer (AACTTCATTATTTCATGCTCCT) [14]. The cycling conditions were the same as the first round PCR except the annealing temperature was set at 48 °C for 45 s. The second round PCR product was run on a 1.5% agarose gel, with an expected band size of approximately 390 bp. Only samples with a visible band were cleaned using the QIAquick PCR purification kit (Qiagen, Germany) protocol as per manufacturer’s instructions.
Sanger sequencing
Sanger sequencing was performed using the foward and reverse primers from the second round PCR and the BigDye™ Terminator 3.1. Cycle Sequencing Kit (Applied Biosystems, United States). For each sample, a total reaction of 10 µl was prepared for each primer, with 5x sequencing buffer, 3.3 μm of primer, 2ul BigDye terminator 3.1, 2ul nuclease-free water and 3ul of purified product. The PCR was run at 96 °C for 1:30 min, 25 cycles of denaturation (96 °C for 30 s), annealing (50 °C for 15 s), and extension (60 °C for 1:30 min). The BigDye XTerminator Purification Kit (Applied Biosystems, United States) was used to purify the DNA and sequencing was run on the 3500xL Genetic Analyser (Applied Biosystems, United States). Sequencher was used to trim and assemble sequences against the reference sequence NC001489 (https://www.ncbi.nlm.nih.gov/nuccore/NC_001489).
Analysis
Aliview 1.27 was used to map and align the consensus sequences against the reference. The aligned sequences were run through the HAV genotyping tool (https://www.rivm.nl/mpf/typingtool/hav/) to identify the genotype. The neighbour-joining distance between the detected strains and previously characterised- (reference) hepatitis strains were computed using the Kimura two-parameter method. The constructed phylogenetic trees were assessed by bootstrap analyses (1000 replicates) and a value of ≥ 70% was considered significant. Nucleotide diversity was calculated using DNA Sequence Polymorphism v6.12.03. The latter software, estimated the intra-population nucleotide diversity by performing pairwise comparison between all sequences.
Results
Incidence of HAV in South Africa
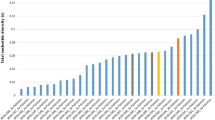
A total of 142 295 samples were tested for anti-HAV IgM across the nine provinces of South Africa. The incidence rate of HAV IgM was 6.28 per 100 000 in South Africa from 1 January to 31 October 2023, with the highest incidence rate observed in Western Cape (15.86/100,000). The HAV positivity rate among the tested population was the highest in Western Cape (0.8%; 1162/142 295), followed by Gauteng (0.5%; 774/142 259) and KwaZulu-Natal (0.5%; 750/142 259). The remaining provinces had a positivity below 0.3%. When comparing Western Cape to positive cases observed in South Africa, the highest positivity was 1.1% [weeks 6 (38/3335), 14 (31/2768), 24 (31/2926), and 26 (36/3298)] and 1.2% [weeks 8 (36/3125), 20 (40/3226), and 29 (40/3357)]. The positivity rate in the Gauteng province was highest durings weeks 42 (1.2%; 42/3567 ) and 44 (0.9%; 12/1316). Whilst in KwaZulu-Natal positivity was greatest during weeks 32 (0.9%; 28/3053), 39 (0.8%; 29/3041) and 42 (0.8%; 28/3567) (Fig. 1).

Hepatitis A cases detected over time in South Africa from January to October 2023, based on seropositive HAV IgM. The bars represent the number of positive cases in each province, and the black line graph the positivity rate
The increase of the number of HAV cases, from January to October 2023, in the Western Cape in relation to other provinces warranted further laboratory investigation. HAV was detected in the 6 districts from which samples were collected from the Western Cape. The incidence rate was calculated using the Western Cape province population data from 2023. The lowest in the City of Cape Town (14.82/100 000), with higher rates in the Cape Winelands, Garden Route, West Coast, Overberg and Central Karoo ranging from 17.15 to 19.73/100 000. When comparing the positivity, the HAV IgM positivity rate was highest in the City of Cape Town Metropolitan district (5.8%; 717/12 347), with a peak in infection observed at weeks 9 (8.5%; 25/293), week 20 (8.7%; 27/310) and week 24 (9.7%; 25/258) (Fig. 2). This was followed by Cape Winelands district with an overall positivity rate of 1.4% (178/12 347), where the highest positivity was observed at week 26 (3.1%; 9/288) and week 39 (3.3%; 7/209). Central Karoo, Garden Route, Overberg, and West Coast districts had a positivity below 1.0%.

The distribution of HAV IgM positives across the six Western Cape districts included in this study period. (A) The number of positive cases detected in the Western Cape districts. (B) The positivity rate detected in each district over time in the Western Cape
Description of outbreak thresholds and HAV incidence in the Western Cape
In the Western Cape, HAV IgM was primarily detected in the age category 5–9 years at 28.0% (325/1162), 16.9% (196/1162) in 10–19 years, and 10.6% (123/1162) in 20–24 years (Table 1). The positivity rate of HAV was similar in males and females, at approximately 50%.
Based on the CuSum2 threshold from 2019 to 2023 in the Western Cape province (Fig. 3A), an increase in HAV IgM positivity exceeded the mean + 2SD threshold in March 2019, January to March 2021 and from February to May 2023, with a peak in March 2023. Across all six districts an increase in positive cases exceeding the mean + 2SD threshold was observed for some years. In 2021, the number of cases increased above the threshold in the West Coast district from January to June (Fig. 3C) and Central Karoo district from January to May (Fig. 3G). The number of cases were above the threshold in the Garden Route district (Fig. 3B) in December 2020 and August 2022, City of Cape Town Metro district from February to April 2022 and from January to March 2023 (Fig. 3D), and in Overberg district in August 2020 and October 2022 (Fig. 3E). In Cape Winelands district, multiple peaks were observed with the number of cases exceeding the CuSum2 threshold in January 2020, November 2022, February and May 2023 (Fig. 3F).

Acute hepatitis A cases by district in South Africa over time from January 2017 to October 2023. Number of hepatitis A cases (blue line) in comparison with threshold (green line), calculated using the CuSum2 method. (A) Western Cape province, (B) Garden Route district, (C) West Coast district (WEC), (D) City of Cape Town Metro (CAT), (E) Overberg district (OVE), (F) Cape Winelands districts (CWL), and (G) Central Karoo district (CKA)
HAV genotypes detected in Western Cape
HAV IgM positive serum samples were received for genotyping from the Western Cape province across the six districts, from 12 March to 07 October 2023 (Fig. 4). The hepatitis A VP1/P2B junction (nucleotide position 2895 bp to 3294 bp) of 150 samples was sequenced to identify the HAV genotype currently circulating. Ninety-three percent (139/150) of hepatitis A seropositive (IgM) samples were successfully sequenced, among which only genotype IB was detected (Fig. 5). The City of Cape Town Metropolitan district had the majority of samples genotyped at 79.9% (111/139). Most of the samples genotyped belonged to persons aged 5–19 years 46.8% (65/139) and 42.4% (59/139) aged 20–34 years (Table 2). When analysing the number of IB sub-genotypes detected in females compared to males, females (39.3%; 59/150) were slightly lower than males (53.3%; 80/150) (Table 2). Majority of our sequences clustered with samples sequenced from the Western Cape, Eastern Cape, KwaZulu-Natal, Gauteng and Limpopo and North West provinces, while approximately 13 sequences clustered with sequence data generated internationally.
Our sequence data were quite scattered across 14 sub-clusters (Fig. 6) within the IB sub-genotype due to a nucleotide diversity of 0.03 (3%) when comparing the VP1/P2B region across the population sequenced. When compared to the reference sequence the diversity of the sequences from this study < 28% (Table S1). Three primary mutations were observed across more than 49% of the samples sequenced: 93.5% (129/139) had R63K (188: G > A) and R71S (213: G > T), and 53.6% (74/139) had M104I (312: G > A) non-synonymous nucleotide changes (Fig. S1).

Map displaying the positive HAV cases in the Western Cape province, from March to October 2023. (A) Map of the Western Cape Province divided by sub-districts. Sub-districts with HAV are represented by the green shaded areas on the map. The size of the red circles is indicative of the number of cases present in that sub-district i.e., the smaller the circle the fewer the cases and the larger the circle the higher the number of cases. (B) Map of the City of Cape Town District and the sub-districts. Each colour on the map represents a different sub-district. The red dots represent the location of the positive HAV cases detected in each sub-district

Neighbour-joining tree displaying the HAV IgM positive cases circulating in the Western Cape province (blue diamonds) and clustering with genotypes used as reference data. The coloured triangles represent compressed portions of the tree that only include reference sequences that cluster with other HAV genotypes (IA, IIA, IIIA, and V). The branch lengths display the nucleotide changes observed in that sequence. Only bootstraps ≥70 are displayed above each branch
Further analysis was performed to determine the relationship between the sub-districts and phylogenetic clustering (Fig. 6). Twenty-two sub-districts were identified among the samples that were successfully genotyped. Majority of samples genotyped were from patients from the Southern sub-district (20.9%; 29/139), Mitchells Plain sub-district (20.9%; 29/139), Western sub-district (17.3%; 24/139), Klipfontein sub-district (7.9%; 11/139), Eastern and Tygerberg sub-districts (5.0%; 7/139), located in close proximity within the City of Cape Town Metropolitan district (Fig. 4). Less than 3% of sequences belonged to each of the remaining sub-districts. Our sequences clustered into fourteen closely related sub-clusters within the IB sub-genotype population. These clusters included samples received from patients residing in various sub-districts and did not solely cluster by sub-districts. Mitchells Plain and the Southern sub-districts were the only sub-districts that clustered in several locations of the phylogentic tree and most commonly occurring in cluster 1 (Fig. 6). This suggests some nucleotide diversity as a result of travelling from one sub-district to another since these sub-districts are located adjacent to each other (Fig. 4). Samples from the Southern sub-district were identified across most of the clusters including 1, 2, 4, 5,6, 7, 8, 11, 12, 13 and 14. Similarly, samples from Mitchells Plain sub-district clustered closely with the Southern sub-district samples in clusters 1, 2, 4, 5, 6, 7, 12, and 14. In addition, samples from Mitchells Plain also clustered in group 9. Samples from the Western sub-district clustered together in groups 2, 3, 4, and 9, with some clustering observed close to samples from the Southern or Mitchells Plain sub-districts. Samples from Klipfontein only clustered together in groups 9 and 14, while the remaining samples from this sub-district was scantily detected with other clusters. The Western sub-district and Klipfontein are also located adjacent to the Southern and Mitchells Plain sub-districts (Fig. 4). Majority of the samples from the Eastern sub-district were identified in cluster 12, while most of the samples from Tygerberg sub-district were identified in cluster 3. The latter suggests a difference in the nucleotide sequence as compared to other clusters from the Southern and Mitchells Plain sub-districts.

Phylogenetic tree displaying the HAV positive cases circulating in the Western Cape province. All nodes with an HAV# (e.g. HAV0072) represent the sequence data from this study. Each node with a shape/colour represents a Western Cape sub-district (as shown in the legend). A node without a shape/colour represents the reference data or for HAV# the sub-district could not be identified. The bracketed regions and numbers represent a cluster
Discussion
HAV is still a global health concern, with higher incidence observed in low to middle income countries, although symptoms are not always evident as a result of partial immunity in endemic countries [15]. Our study has confirmed the increased HAV positivity rate in the tested population and the genotype clusters in Western Cape in 2023 using SDW and NMCSS data with additional laboratory investigation. Using the CuSum2 threshold to monitor HAV, we were able to identify the sudden increase and suspected HAV outbreak in two districts in the Western Cape province in 2023, with HAV cases above the threshold in the City of Cape Town and the Cape Winelands districts. Overall, the highest incidence was detected in the Western Cape province among the children aged 5 to 14 years. Sixty-one percent of patients infected with HAV resided in the City of Cape Town Metropolitan district, which was higher than observed in all other districts.
The HAV sub-genotype 1B strain circulating in the City of Cape Metropolitan relates to the HAV strain detected previously in South Africa [4, 6, 16, 17]. The IB sub-genotype was previously reported to occur more often among patients with acute liver failure [18], however the true relationship between clinical presentation and HAV genotypes is not well elucidated. HAV has a low diversity rate which was evident from our sequence data where few minor amino acid changes were evident from different patient samples. Usually HAV detected around the same geographic area cluster with strains of similar genetic phylogeny may indicate an endemic transmission pattern or viral fitness advantage in that region [19]. This seems to be the case in the City of Cape Town sub-districts where common mutations such as R63K, R71S and M104I were detected across different patient samples. R63K in the VP1/P2B region is similar to R298K mutation in the VP1 region [20]. This mutation does not affect the protein structure of VP1 nor does it impact the antigenic stability of the virus [14]. R71S was previously detected in sub-genotype IB in wastewater samples in South Africa, although its function has not been reported [20]. The M104I has also been observed in sub-genotypes IIIA and IIIB [20].
Similar to the NMCSS analysis where majority of HAV IgM positives were observed in the City of Cape Town district, the HAV genotypes were predominantly detected in the City of Cape Town district. The transmission of HAV within the City of Cape Town district was clearly established although the source of transmission was uncertain. Large clusters of cases were observed geographically in the Southern sub-district, Mitchells Plain sub-district, and the Western sub-district, which are urbanised and comprise some of the wealthiest sub-districts in the Western Cape [21]. The City of Cape Town district has the highest population (64.2% in 2022) compared to other districts in the Western Cape [22], which suggests transmission between sub-districts. In addition, the City of Cape Town district also has the highest proportion of people living in poverty when compared with other districts in the Western Cape province, which also suggests areas with poor sanitation that could contribute to the transmission of HAV [23].
A primary limitation of this study was that the source of the transmission could not be identified due to lack of epidemiological information. The NMCSS data has the capability of updating the clinical and epidemiological information but some of the information was missing and therefore analysis of risk factors could not be included. Awareness of the opportunity to update the information should be done regularly in order for the user to improve data completeness needed for public health analysis. A second limitation was that we did not have sufficient data on the patients’ medical history and other viral factors that may have contributed to infection to determine the severity of disease and its possible relationship with the HAV genotypes. Lastly, there is a gap in the geographical distribution of samples sequenced in our study. This study only received IgM serologically positive HAV samples from the NHLS laboratory in Groote Schuur; the laboratory tests more samples from the City of Cape Town Metropolitan district compared to other districts in Western Cape. Future analysis will need to be done to include samples from NHLS laboratories in Tygerberg and George, as well as the private laboratories.
In conclusion, genotyping can assist with identifying clusters of outbreaks, especially if coupled with epidemiological and geographical data. However, South Africa requires the implementation of active surveillance to effectively target the areas of high prevalence to identify the HAV risk factors. This will allow for more rapid public health responses and implementation of preventative measures such as the HAV vaccine roll-out in the future. In light of the evidence that HAV seropositivity is < 90% in children under 10 years of age showing the transition from high to intermediate endemicity in South Africa, it is recommended to administer routine HAV vaccination to children from 2 years of age, through the national EPI in South Africa [6]. The HAV vaccine is only available in the private sector which makes the transmission of infection within communities with low immunity at high risk in South Africa.
Data availability
The datasets generated and/or analysed during the current study are available in the National Library of Medicine (https://www.ncbi.nlm.nih.gov/) GenBank repository, accession numbers include PP828805-PP828943.
References
Patterson J, Abdullahi L, Hussey GD, Muloiwa R, Kagina BM. A systematic review of the epidemiology of hepatitis A in Africa. BMC Infect Dis. 2019;19:1–15.
Jefferies M, Rauff B, Rashid H, Lam T, Rafiq S. Update on global epidemiology of viral hepatitis and preventive strategies. World J Clin Cases. 2018;6:589–99.
Nainan OV, Xia G, Vaughan G, Margolis HS. Diagnosis of Hepatitis A Virus infection: a Molecular Approach. Clin Microbiol Rev. 2006;19:63–79.
Mazanderani AH, Motaze NV, McCarthy K, Suchard M, du Plessis NM. Hepatitis A virus seroprevalence in South Africa - estimates using routine laboratory data, 2005–2015. PLoS ONE. 2018;14(6):2005–15.
NICD, Communicable Diseases, Communique. January. 2023, vol.22(1). Vol. 22. 2023.
Enoch A, Hardie DR, Hussey GD, Kagina BM. Hepatitis A seroprevalence in Western Cape Province, South Africa: are we in epidemiological transition? South Afr Med J. 2019;109:314–8.
Plessis NM, Mazanderani AH, Motaze NV, Ngobese M, Avenant T. Hepatitis A virus seroprevalence among children and adolescents in a high – burden HIV setting in urban South Africa. Sci Rep. 2022;12:1–6.
Prabdial-Sing N, Motaze V, Manamela J, McCarthy K, Suchard M. Establishment of outbreak thresholds for hepatitis a in South Africa using laboratory surveillance, 2017–2020. Viruses. 2021;13:2017–20.
McKnight KL, Lemon SM. Hepatitis a virus genome organization and replication strategy. Cold Spring Harbor Perspect Med. 2018;8:1–18.
Averhoff FM, Khudyakov Y, Nelson NP, Hepatitis A. Vaccines. Seventh Ed. Plotkin’s vaccines. Elsevier Inc.; 2017. pp. 319–e34115.
Costa-Mattioli M, Di Napoli A, Ferré V, Billaudel S, Perez-Bercoff R, Cristina J. Genetic variability of hepatitis a virus. J Gen Virol. 2003;84:3191–201.
Malhotra B, Kanwar A, Reddy PVJ, Chauhan A, Tiwari J, Bhargava S, et al. Molecular characterization of hepatitis a virus from children hospitalized at a tertiary care centre in northwest India. Indian J Med Res. 2018;147:507–12.
Averhoff F, Khudyakov Y, Vellozzi C. 174 - Hepatitis A Virus. Ninth edit. Mandell, Douglas, and Bennett’s principles and practice of Infectious diseases. Elsevier Inc.; 2017. pp. 2243–61.
Rachida S, Wolfaardt M, Taylor MB. Molecular characterisation of hepatitis a virus strains from water sources in South Africa. Water Sci Technol. 2014;69:923–33.
Abutaleb A, Kottilil S, Hepatitis A. Epidemiology, natural history, unusual clinical manifestations, and Prevention. Gastroenterol Clin N Am. 2020;49:191–9.
Newman H, Tshabalala D, Estrada GAP, Newman H, Tshabalala D, Estrada GAP, et al. Hepatitis A in Nelson Mandela Bay and Sarah Baartman districts, Eastern Cape, South Africa. South Afr J Infect Dis. 2018;0:1–4.
Taylor MB. Molecular epidemiology of South African strains of hepatitis a virus: 1982–1996. J Med Virol. 1997;51:273–9.
CDC, Hepatitis A, Virus Infections. :FAQS. 2008;1–2.
Wang H, Zheng H, Cao J, Zhou W, Yi Y, Jia Z, et al. Genetic diversity of Hepatitis A Virus in China: VP3- VP1-2A genes and evidence of quasispecies distribution in the isolates. PLoS ONE. 2013;8:1–9.
Rachida S, Taylor MB. Potentially infectious novel hepatitis a virus strains detected in selected treated wastewater discharge sources, South Africa. Viruses. 2020;12:1468.
Statistics South Africa. Section B: Profile Western Cape Province. 2020.
Department: Statistics South Africa. Republic of South Africa. Consensus 2022. 2024. stat sa. https://census.statssa.gov.za/#/province/1/2 (accessed 06 March 2024).
Western Cape Government. #KnowYourMunicipality: The Socio-Economic Profile. City of Cape Town. 2022. pp. 1–22 City of Cape Town.
Acknowledgements
Thank you to Tshepo Motsamai from the NICD, CVI for assisting with populating the relevant NMC and SDW datasets and merging the genotyping datasets with corresponding datasets. Thanks to the Western Cape Province Health Department for the population data generated and district/sub-district level data made available for this study. Lastly, thank you to the NHLS, Groote Schuur Laboratory staff for preparing the samples for shipment to the NICD for testing and ensuring samples reached our laboratory timeously.
Funding
Funding for this study was acquired through the National Health Laboratory Service which provides core funding for surveillance activities performed at the Centre for Vaccines and Immunology, NICD.
Author information
Authors and Affiliations
Contributions
K. S. and N. P.S. contributed to the conceptualization of the manuscript.K.S. drafted the main manuscript text, analysed and interpreted the data.K.S., J. M., S. K, J.B., C.L., J.T., K.B., J.K., and Z.K. contributed to the acquisition of data. J.K., and Z.K. prepared Fig. 4. J.M. prepared data for Fig. 3. K.S. agrees to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.All authors have reviewed and approved the submitted version.
Corresponding author
Ethics declarations
Ethical approval
The study was performed in accordance with the ethical standards as per the 1964 Declaration of Helsinki (updated in October 2013). Ethical approval for the use of data and investigations on notifiable medical conditions was obtained from the Human Research Ethics Committee of the University of Witwatersrand (Ethical Clearance Number: M210752). The need for consent to participate was waived as per the Institutional Review Board (IRB) Human Research Ethics Committee of the University of Witwatersrand (Ethical Clearance Number: M210752) and deemed necessary according to the National Health Act, 2003, Chap. 3: Prevention and Control of communicable diseases by health authorities and heads of institutions.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Subramoney, K., Manamela, J., Korsman, S. et al. Molecular characterisation of hepatitis A in the Western Cape province, South Africa in 2023. BMC Infect Dis 24, 845 (2024). https://doi.org/10.1186/s12879-024-09738-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09738-7