
Abstract
Background
Pulmonary abscesses resulting from epididymitis caused by extended spectrum β-lactamase-producing hypervirulent Klebsiella pneumoniae (ESBL-hvKp) in a nondiabetic patient are extremely uncommon. The infection caused by this disseminated drug-resistant bacteria, which is generally considered an intractable case, poses a potential challenge in clinical practice.
Case presentation
In this case report, we present the clinical course of a 71-year-old male patient with epididymitis, who subsequently developed cough and dyspnea following anti-infection treatment. Imaging examinations revealed severe pneumonia and pulmonary abscess. The infection of ESBL-hvKp in the epididymis led to bacteremia and subsequent lung lesions. Due to poor response to anti-infection therapy, the patient required an extended duration of anti-infection treatment and ultimately chosed to discontinue treatment.
Conclusions
Acute epididymitis caused by ESBL-hvKP infection can result in the spread of the infection through the bloodstream, leading to severe pneumonia and lung abscess. Given the critical condition of the patient, even with active anti-infection treatment, there is a risk of treatment failure or potentially fatal outcomes.
Similar content being viewed by others


Introduction
Acute epididymitis is commonly caused by bacteria such as Escherichia coli, staphylococcus, enterococcus, and streptococcus faecalis. However, it is extremely rare for it to be caused by extended spectrum β-lactamase-producing hypervirulent Klebsiella pneumoniae (ESBL-hvKp). We present a recent case of a patient with acute epididymitis caused by ESBL-hvKp, leading to the development of metastatic severe pneumonia and pulmonary abscesses formation from hematogenous seeding of an infectious source located distally. Despite receiving 20 days of anti-infective therapy, the patient remained in poor condition, and they decided to discontinue treatment and was subsequently discharged.
Case presentation
The patient is a 71-year-old male with a history of hypertension for the past ten years. He had been receiving drug treatment and was able to maintain a normal lifestyle. Three months prior to admission, he underwent electroprostatectomy due to prostatic hyperplasia. The patient initially presented to our hospital with a 5-day history of pain and swelling in the right scrotum, accompanied by a 1-day history of high-grade fever reaching 39 °C. Physical examination revealed right testicular edema with pain upon palpation of the epididymis, and a hard mass measuring 4 cm×2 cm was detected. Poor demarcation was observed between the testicle and epididymis. Laboratory tests showed abnormal results, including a white blood cell count (WBC) of 26.06 (normal range: 3.5–9.5 × 109/L) with 93.1% neutrophils (normal range: 40.0–75.0%), elevated C-reactive protein (CRP) level of 230.96 mg/dl (normal range: ≤0.5 mg/dl), and Procalcitonin (PCT) level of 16.54 ng/ml (normal range: ≤0.5 ng/dl). Slightly elevated total bilirubin (TBIL) of 34.6 umol/l (normal range: 0–26 umol/l) and direct bilirubin (DBIL) of 25.18 umol/l IU/L (normal range: 0–8 umol/l) were also observed. Scrotal ultrasound revealed an enlarged right epididymis with mildly increased vascularity on color Doppler, consistent with epididymitis (Fig. 1).

Scrotal Ultrasound. The right epididymis associated with an enlargement in size and vascularization (blue and red signal)
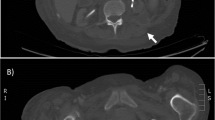
The patient was diagnosed with acute epididymitis and admitted to the urology ward for further evaluation and treatment. Empiric antibiotic therapy with intravenous ceftazidime (2 g every 8 h) and metronidazole (500 mg every 8 h) was initiated. 2 days after admission, the patient began experiencing occasional dry cough. Chest x-ray revealed scattered bilateral patchy ground-glass opacity and pulmonary nodules with some cystic cavities, and small left-sided pleural effusion (Fig. 2A). Computed tomography (CT) scan of the chest showed bilateral lung inflammation and pulmonary abscesses (bilateral pulmonary nodules with central cavitation), enlargement of mediastinal lymph nodes, and small bilateral pleural effusion (Fig. 3A and B).

Chest X-ray. (A) Scattered bilateral patchy ground-glass opacity and pulmonary nodules with some cystic cavities, and small left-sided pleural effusion; (B) more bilateral patchy ground-glass opacity and small left-sided pleural effusion; (C)extensive bilateral patchy ground-glass opacity with multiple pulmonary cavities, and small bilateral pleural effusion
Glycosylated hemoglobin assay, autoimmune antibody and HIV testing, molecular assay for tuberculosis, and a transthoracic echocardiogram, were conducted, yielding no significant abnormalities in the findings. The patient was supplementally diagnosed with pneumonia and pulmonary abscess.
On the 4th day of hospitalization, the patient’s condition worsened, with increased respiratory symptoms and oxygen saturation dropping to 89–92% on room air. As a result, the patient was transferred to the intensive care unit (ICU) for further treatment. High flow nasal cannula (HFNC) was employed to alleviate dyspnea, resulting in improved oxygen saturation levels of 96 to 98%. Despite the initial negative results of the blood and urine bacteriological cultures obtained on the first day of admission, we thinked that the patient was suffering from epididymitis and suspected that the bacteria had spread to the bloodstream, leading to pneumonia and lung abscesses. Given the poor response to the initial empirical antibiotic agents, the decision was made to discontinue ceftazidime and metronidazole and instead initiate intravenous piperacillin-tazobactam (4.5 g every 8 h) and moxifloxacin (0.4 g once daily). 6 days after admission, a repeat chest CT scan revealed similar amounts of exudation, but with more multiple lung cavity lesions than the previous scan. Mediastinal lymph nodes enlargement and small bilateral pleural effusion were still present (Fig. 3C and D). The patient continued to experience intermittent fever, with a maximum body temperature of 39.5 °C. Blood culture results identified gram-negative bacilli, and extended-spectrum β-lactamase-producing Klebsiella pneumoniae (ESBL-Kp) was reported as the positive culture the following day. The isolate’s susceptibility was tested using minimal inhibitory concentration (MIC) test strips, and it was found to be susceptible to amikacin (MIC ≤ 4), minocycline (MIC ≤ 4), imipenem (MIC ≤ 1), meropenem (MIC ≤ 1), and tigecycline (MIC ≤ 2). Consequently, piperacillin-tazobactam and moxifloxacin were discontinued, and the patient’s infection control regimen was adjusted to include imipenem (1 g every 6 h intravenously) and minocycline (0.1 g every 12 h orally) after 6 days of antibiotic therapy.
On the 8th day after admission, the patient developed hypoxemic respiratory failure and required endotracheal intubation. The culture of bronchoalveolar lavage fluid (BALF) yielded the same ESBL-Kp organism the following day. The patient was thus diagnosed with pulmonary abscess secondary to epididymitis caused by ESBL-Kp. On the tenth day, repeat laboratory investigations revealed a WBC of 5.41 × 109/L with 80% neutrophils, CRP level of 190.05 mg/dl, and PCT level of 1.79 ng/ml. Repeat chest x-ray showed more bilateral patchy ground-glass opacity and similar small left-sided pleural effusion than previous x-ray(Fig. 2B).
Due to the severe infection, the patient was transferred to the intensive care unit (ICU) at Zhujiang Hospital of Southern Medical University, 11 days after admission. Antibiotic treatment in the ICU included intravenous meropenem (1 g every 6 h) and tigecycline (0.1 g every 12 h). During the patient’s ICU stay, imaging studies were repeated, and a CT scan showed an increase in exudation and in the number of multiple pulmonary cavity lesions than previous scans (Fig. 3E, F). A scrotal ultrasound revealed the presence of a right testicular abscess and epididymal abscess. The urologist recommended a review of the scrotal ultrasound after a week of anti-inflammation treatment, and drainage of the abscesses if necessary. Follow-up chest x-ray indicated extensive bilateral patchy ground-glass opacity with multiple pulmonary cavities, and small bilateral pleural effusion (Fig. 2C). Additionally, the scrotal ultrasound confirmed the presence of right testicular and epididymal abscesses, as well as bilateral epididymitis. Surgical intervention was suggested, but the patient declined further treatment. The patient’s oxygen levels remain low, and the tracheal intubation cannot be removed. As a rest, the patient chosed to be discharged after 20 days of antibiotic therapy. It’s important to note that discontinuing treatment can lead to worsened illness and potentially death.

Computed tomography (CT) scan of the chest. (A, B) Bilateral pulmonary nodules with central cavitation representing pulmonary abscesses; (C, D) multiple pulmonary nodules with central cavitation; (E, F) numerous large cavitary lesions representing multifocal pulmonary abscesses
The Klebsiella pneumoniae (K. pneumoniae) isolate was extensively studied at the Laboratory of Respiratory Disease in People’s Hospital of Yangjiang, China. Capsular genotyping, a combination of the Galleria mellonella killing assay and a string test, virulence gene testing, and multilocus sequencing typing (MLST) were performed. The isolate was identified as a sequence type 23 serotype K1 strain (ST23-K1), carrying virulence-associated genes such as rmpA, magA, and aerobactin, but was negative for rmpA2. Furthermore, both the Galleria mellonella killing assay and string test produced positive results. Therefore, the clinical presentation and laboratory findings support categorizing the infection as a disseminated infection with hypervirulent K. pneumoniae (hvKp).
Discussion
Acute epididymitis is a common urological emergency characterized by redness, swelling, and pain in the scrotum, often accompanied by fever and chills. In recent years, K. pneumoniae infections causing epididymitis and epididymal abscesses have been increasingly reported [1]. Acute epididymitis can occur through retrograde, hematogenous, lymphatic, and other routes, and is frequently secondary to urinary tract infections, long-term indwelling urinary catheters, invasive urethral procedures, urethral strictures, and obstructions. Conservative treatment, including aggressive and effective antimicrobial therapy for an extended period, is often the primary approach for acute epididymitis, with favorable outcomes in most patients. However, if ultrasound reveals the presence of epididymal abscess or testicular vascular disorders, accompanied by severe scrotal pain and high fever, prompt surgical intervention for drainage becomes necessary. In cases where testicular necrosis is observed, the testis and epididymis may need to be surgically removed. In the present case, the patient had recently undergone electroprostatectomy, which was considered a factor contributing to the backward flow of urine into the ejaculatory ducts, retrograde bacterial infection, or impaired semen discharge due to ejaculatory duct damage. Subsequently, the patient developed epididymitis.
This case involves a community-acquired infection. The clinical presentation and findings from blood and sputum cultures suggested that the epididymitis was caused by ESBL-hvKP. The bacteria had invaded the bloodstream, resulting in severe pneumonia and lung abscesses.It is worth noting that reports of pulmonary abscesses secondary to epididymitis caused by K. pneumoniae, especially ESBL-hvKP, are exceedingly rare.
K.pneumoniae is classified under the Enterobacteriaceae family. Currently, there are two main pathotypes of K. pneumoniae that are spreading globally: classical K. pneumoniae (cKP) and hypervirulent K. pneumoniae (hvKP). The majority of hvKP infections are acquired within the community. hvKp can infect multiple sites of the body at the same time. This is usually characterized by a rapidly metastatic spread, leading to the development of hepatic abscesses, meningitis, brain abscesses, lung abscesses, endophthalmitis, and necrotizing fasciitis, and this is collectively referred to as Klebsiella pneumoniae invasive syndrome (KPIS). [2, 3]. KPIS was initially reported in Taiwan in the 1980s, and since then, the incidence of hvKP infection has been steadily increasing. The occurrence of hvKP infections is now geographically widespread, although it is more prevalent in immunocompromised individuals of Asian Pacific Rim [4, 5]. The reasons for this regional prevalence remain unclear and may be influenced by various ethnicities and environmental factors. It is noteworthy that the age of onset of the disease is not limited to the elderly, as healthy individuals of any age can be affected. hvKP strains have been found to be uniformly resistant to ampicillin, but their resistance to other antimicrobial drugs is generally lower compared to traditional K.pneumoniae strains.
Laboratory tests have been used to define hvKp. One of the factors contributing to its virulence is the enhanced polysaccharide capsule, and most cases of hvKp produce capsules of serotype K1, K2 [6,7,8]. Previous studies have shown that ST23 is the most prevalent sequence type (ST) in hvKp isolates and strongly correlates with the K1 capsular serotype [9]. Currently, the recommended definitive diagnostic tests for hvKp involve the detection of virulence-associated genes such as aerobactin or a combination of the Galleria mellonella killing assay and the string test [10, 11]. Regulatory genes like rmpA and rmpA2 increase capsule polysaccharide production and the hypermucoviscous phenotype; the mucoviscosity-associated gene A (magA), which encodes an enzyme, has also been found to contribute to the hypervirulent phenotype [6, 7]. Aerobactin has been identified as a major virulence factor in hvKp isolates due to its association with increased siderophore production [10]. The hypermucoviscous phenotype can also be detected using the “string test,” which is positive when a bacterial colony can be stretched more than 5 mm from the agar plate [6]. Furthermore, the combination of the Galleria mellonella killing assay and the string test has a sensitivity of 95.56% and a specificity of 94.83%, making it a relatively simple and accurate method to identify clinical hvKp isolates [11]. The present study confirms that disseminated infection is due to hypervirulent K. pneumoniae (ST23-K1).
Cheng et al. reported a case of septic pulmonary embolism secondary to K. pneumoniae epididymitis [12]. Additionally, Ojeda et al. identified another case of this condition [13]. The similarities between the two cases include epididymitis with the isolation of K. pneumoniae, multiple bilateral nodular lesions with pleural effusion, and a history of diabetes. However, the hvKp strains in these two cases were found to be antimicrobial sensitive, not resistant to antimicrobials. Wen et al. reported a case of right epididymitis caused by multidrug-resistant Klebsiella pneumoniae (KPI), but no metastatic spread was observed, suggesting that this bacteria may be less virulent [14]. Generally, drug-resistant hvKp infections in the community are rare. In our study, we found that the K. pneumoniae infection in this immunocompetent patient produced an ESBL enzyme, which eventually metastasized and caused severe pneumonia, followed by a pulmonary abscess. The patient required endotracheal intubation and ventilator-assisted breathing. Unfortunately, the patient did not respond well to antibiotic treatment, and extended administration of anti-infection regimens was necessary. Ultimately, the patient decided to discontinue treatment and was discharged. Therefore, for patients with acute epididymitis, it is important to be vigilant about the possibility of secondary severe pneumonia and lung abscess, especially if symptoms such as cough, sputum, chest tightness, and low oxygen saturation occur during the course of the disease. Prompt and effective anti-infection measures are crucial as delay in treatment can often pose a threat to the patient’s life.
Some aspects of treatment failure should be taken into consideration. Delaying medical attention for five days after the onset of illness can have negative consequences on the prognosis of the patient. In cases of infectious diseases, timely intervention is crucial. The accurate judgment of the patient’s condition by the doctor and the adjustment of treatment methods play a significant role in the patient’s recovery. Generally, hvKp is more commonly associated with community-acquired infections compared to cKP. However, drug-resistant bacteria are rare, and in this particular case, the K. pneumoniae is producing ESBL enzymes, leading to a limited response to anti-infection treatment. Seeking medical attention promptly can potentially improve the prognosis of this patient by strengthening the anti-infection treatment. Due to the high prevalence of ESBL-producing bacteria in China, patients should be treated with antimicrobial agents containing enzyme inhibitors, such as piperacillin-tazobactam or cefoperazone-sulbactam, instead of ceftazidime, at an early stage. This highly virulent bacterium has caused bacteremia and lung abscesses, and an effective approach would involve the administration of intravenous meropenem combined with intravenous tigecycline. Appropriate treatment adjustments based on the patient’s condition and pathogen characteristics are crucial for a successful outcome. If the treatment response remains inadequate, it is advisable to perform prompt drainage of the epididymal abscess. Secondary severe pneumonia and lung abscess necessitate long-term anti-infection treatment. If the patient undergo operation, such as testicular and epididymal surgery, and continues with persistent anti-infection treatment, there is still a possibility for recovery.
Conclusion
Acute epididymitis caused by ESBL-hvKP infection can result in the spread of the infection through the bloodstream, leading to severe pneumonia and lung abscess. Given the critical condition of the patient, even with active anti-infection treatment, there is a risk of treatment failure or potentially fatal outcomes.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Tan J, Tian M, Zhao F, Deng S, Jin P, Wang Y, Wen H, Qin X, Gong Y. An investigation of the male genitourinary abscess originated from urinary tract in a Tertiary Hospital, Shanghai, China, from 2004 to 2019. Infect Drug Resist. 2021;14:1795–803. https://doi.org/10.2147/IDR.S298250. PMID: 34017185; PMCID: PMC8131006.
Namikawa H, Yamada K, Fujimoto H, Oinuma KI, Tochino Y, Takemoto Y, Kaneko Y, Shuto T, Kakeya H. Two unusual cases of successful treatment of hypermucoviscous Klebsiella pneumoniae invasive syndrome. BMC Infect Dis. 2016;16(1):680. https://doi.org/10.1186/s12879-016-2011-3. PMID: 27852233; PMCID: PMC5112683.
Sun R, Zhang H, Xu Y, Zhu H, Yu X, Xu J. Klebsiella pneumoniae-related invasive liver abscess syndrome complicated by purulent meningitis: a review of the literature and description of three cases. BMC Infect Dis. 2021;21(1):15. https://doi.org/10.1186/s12879-020-05702-3. PMID: 33407192; PMCID: PMC7788956.
Lin YT, Cheng YH, Chuang C, Chou SH, Liu WH, Huang CH, Yang TC, Kreiswirth BN, Chen L. Molecular and clinical characterization of Multidrug-resistant and hypervirulent Klebsiella pneumoniae strains from Liver Abscess in Taiwan. Antimicrob Agents Chemother. 2020;64(5):e00174–20. https://doi.org/10.1128/AAC.00174-20. PMID: 32152079; PMCID: PMC7179640.
Harada S, Aoki K, Yamamoto S, Ishii Y, Sekiya N, Kurai H, Furukawa K, Doi A, Tochitani K, Kubo K, Yamaguchi Y, Narita M, Kamiyama S, Suzuki J, Fukuchi T, Gu Y, Okinaka K, Shiiki S, Hayakawa K, Tachikawa N, Kasahara K, Nakamura T, Yokota K, Komatsu M, Takamiya M, Tateda K, Doi Y. Clinical and molecular characteristics of Klebsiella pneumoniae isolates Causing Bloodstream infections in Japan: occurrence of Hypervirulent infections in Health Care. J Clin Microbiol. 2019;57(11):e01206–19. https://doi.org/10.1128/JCM.01206-19. PMID: 31434721; PMCID: PMC6812994.
Choby JE, Howard-Anderson J, Weiss DS. Hypervirulent Klebsiella pneumoniae - clinical and molecular perspectives. J Intern Med. 2020;287(3):283–300. https://doi.org/10.1111/joim.13007. Epub 2019 Nov 21. PMID: 31677303; PMCID: PMC7057273.
Martin RM, Bachman MA. Colonization, infection, and the Accessory Genome of Klebsiella pneumoniae. Front Cell Infect Microbiol. 2018;8:4. https://doi.org/10.3389/fcimb.2018.00004. PMID: 29404282; PMCID: PMC5786545.
Zhang Y, Zhao C, Wang Q, Wang X, Chen H, Li H, Zhang F, Li S, Wang R, Wang H. High prevalence of Hypervirulent Klebsiella pneumoniae infection in China: Geographic distribution, clinical characteristics, and Antimicrobial Resistance. Antimicrob Agents Chemother. 2016;60(10):6115–20. https://doi.org/10.1128/AAC.01127-16. PMID: 27480857; PMCID: PMC5038323.
Guo Y, Wang S, Zhan L, Jin Y, Duan J, Hao Z, Lv J, Qi X, Chen L, Kreiswirth BN, Wang L, Yu F. Microbiological and clinical characteristics of Hypermucoviscous Klebsiella pneumoniae isolates Associated with Invasive infections in China. Front Cell Infect Microbiol. 2017;7:24. https://doi.org/10.3389/fcimb.2017.00024. PMID: 28203549; PMCID: PMC5286779.
Russo TA, Olson R, Macdonald U, Metzger D, Maltese LM, Drake EJ, Gulick AM. Aerobactin mediates virulence and accounts for increased siderophore production under iron-limiting conditions by hypervirulent (hypermucoviscous) Klebsiella pneumoniae. Infect Immun. 2014;82(6):2356–67. https://doi.org/10.1128/IAI.01667-13. Epub 2014 Mar 24. PMID: 24664504; PMCID: PMC4019165.
Li G, Shi J, Zhao Y, Xie Y, Tang Y, Jiang X, Lu Y. Identification of hypervirulent Klebsiella pneumoniae isolates using the string test in combination with Galleria mellonella infectivity. Eur J Clin Microbiol Infect Dis. 2020;39(9):1673–9. https://doi.org/10.1007/s10096-020-03890-z. Epub 2020 Apr 21. PMID: 32318968.
Cheng FY, Su YJ. Septic Pulmonary Emboli Associated with Klebsiella Pneumoniae Epididymitis. J Emerg Med. 2016;50(1):e23–4. https://doi.org/10.1016/j.jemermed.2015.03.044. Epub 2015 Oct 9. PMID: 26443643.
Ojeda Gómez JSA, Carrillo Bayona JA, Morales Cifuentes LC. Septic pulmonary embolism secondary to Klebsiella pneumoniae Epididymitis: Case Report and Literature Review. Case Rep Radiol. 2019;2019:5395090. https://doi.org/10.1155/2019/5395090. PMID: 31016062; PMCID: PMC6444252.
Li YM, Milikowski C, Selvaggi G, Abbo LM, Skiada D, Galimberti F. Polymyxin B-induced skin hyperpigmentation. Transpl Infect Dis. 2020;22(5):e13312. https://doi.org/10.1111/tid.13312. Epub 2020 May 27. PMID: 32386075.
Acknowledgements
The authors thank the patient’s family for their consent to participatein this study. We also appreciate all medical staff’s cooperation and care of the patient.
Funding
This work was not supported by external funding.
Author information
Authors and Affiliations
Contributions
All of the authors contributed to the conception and design of the work. Runjun Li, Liye Yang, and Ling Rong, along with Gang Chen, were responsible for writing the main manuscript texe. Junlong Liu prepared Figs. 1, 2 and 3. Zhiwei Lin conducted molecular research on the Klebsiella pneumoniae isolate in the laboratory. All of the authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work. Additionally, Xiuying Tang, as the corresponding author, has overall supervision and coordination responsibilities for the study, ensuring its integrity and accuracy.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional clinical ethics committee of the People’s Hospital of Yangjiang.
Consent for publication
Written informed consent was obtained from the patient’s family for publication of this report and any accompanying images.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, R., Liu, J., Yang, L. et al. Pulmonary abscess secondary to epididymitis caused by extended spectrum β-lactamase-producing hypervirulent Klebsiella pneumoniae: a case report. BMC Infect Dis 24, 820 (2024). https://doi.org/10.1186/s12879-024-09721-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09721-2