
Abstract
Background
The COVID-19 has been shown to have negative effects on the cardiovascular system, but it is unclear how long these effects last in college students. This study aimed to assess the long-term impact of COVID-19 on arterial stiffness, endothelial function, and blood pressure in college students.
Methods
We enrolled 37 college students who had been infected with COVID-19 for more than 2 months. Brachial artery flow-mediated dilation (FMD) was used to assess endothelial function, while arterial stiffness was evaluated using the ABI Systems 100, including variables such as ankle-brachial index (ABI), brachial-ankle pulse wave velocity (baPWV), carotid-femoral pulse wave velocity (cfPWV), heart rate (HR), and blood pressure (BP).
Results
Our results showed that FMD was significantly impaired after COVID-19 infection (p < 0.001), while cfPWV and systolic blood pressure (SBP) were significantly increased (p < 0.05). Simple linear regression models revealed a significant negative correlation between post-COVID-19 measurement time and baPWV change (p < 0.01), indicating an improvement in arterial stiffness over time. However, there was a significant positive correlation between post-COVID-19 measurement time and diastolic blood pressure (DBP) change (p < 0.05), suggesting an increase in BP over time. There were no significant differences in ABI and HR between pre- and post-COVID-19 measurements, and no significant correlations were observed with other variables (p > 0.05). Conclusion: Our study demonstrated that COVID-19 has long-term detrimental effects on vascular function in college students. However, arterial stiffness tends to improve over time, while BP may exhibit the opposite trend.
Similar content being viewed by others


Introduction
In December 2019, the first case of infection and mortality caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was reported in Wuhan, China [1]. Since then, the virus has spread globally, causing a pandemic. On December 7, 2022, China lifted all restrictions and many individuals who had not previously been infected with coronavirus disease 2019 (COVID-19) were subsequently infected. As of July 26, 2023, there have been 773,511,195 confirmed cases of COVID-19 worldwide, with 7,023,127 deaths reported [2]. In the past, the focus was primarily on the acute adverse effects of COVID-19 on the human body, but evidence suggests that it can have long-term detrimental impacts on individuals after infection [3]. In October 2021, the World Health Organization released a clinical case definition for the post-COVID-19 condition as symptoms that present 3 months after SARS-CoV-2 infection with a minimal duration of 2 months and cannot be explained by an alternative diagnosis [4]. Common symptoms include, but are not limited to, fatigue, shortness of breath, and cognitive dysfunction, and generally have an impact on everyday functioning [4].
The COVID-19 virus has been shown to have adverse effects on vascular function. Abbasi et al. demonstrated that patients experienced a range of increased cardiovascular risks one year after COVID-19 infection [5]. SARS-CoV-2 can invade the human body by binding to angiotensin-converting enzyme 2 (ACE2) receptors expressed in various tissues [6]. The binding of SARS-CoV-2 to ACE2 expressed in vascular endothelium can result in endothelial damage [7]. Previous studies have shown that the degree of arterial stiffness in elderly individuals with COVID-19 worsens during the acute phase and four months after infection, with impaired endothelial function [8, 9]. For the younger population, previous studies have indicated that COVID-19 has no impact on vascular and cardiac autonomic function in young adults [10]. However, there is also evidence suggesting that young individuals infected with COVID-19 experience increased arterial stiffness [11]. Arterial stiffness is closely related to vascular aging, and an increase in arterial stiffness is considered as an early marker for vascular aging [12]. The European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) recommend the use of pulse wave velocity (PWV) as a comprehensive and non-invasive measurement method for assessing arterial stiffness, as it is sufficiently simple and accurate [13]. PWV has been widely used as the gold standard for assessing arterial stiffness in clinical practice [14]. Vascular aging is also characterized by elevated systolic blood pressure (SBP), which is attributed to impaired generation and repair function of the vascular endothelium, leading to endothelial aging and associated vascular dysfunction, ultimately increasing the risk of cardiovascular diseases [15]. Brachial artery flow-mediated dilation (FMD), a non-invasive method for assessing endothelial function, has been widely used as an alternative marker for endothelial dysfunction in various clinical conditions such as asymptomatic atherosclerosis, coronary artery disease (CAD), congestive heart failure (CHF), and other cardiovascular diseases [16].
Currently, there is no research investigating the long-term effects of COVID-19 infection on vascular function in college students.
This study discovered significant alterations in endothelial function, arterial stiffness, and blood pressure levels among college students during the 2- to 5-month period following COVID-19 infection.
Patients and methods
Study design
This study utilized a pre-post design to assess the long-term effects of COVID-19 infection on vascular function in college students. Vascular endothelial function, arterial stiffness, and blood pressure were recorded before and after COVID-19 infection. All pre-COVID-19 measurements were conducted between September 20th and September 24th, 2022, and post-COVID-19 measurements were conducted between February 2023 and June 2023 at Guangdong Provincial Key Laboratory of Physical Activity and Health Promotion, Guangzhou Sport University. The same measurement protocol as before COVID-19 infection was employed after COVID-19 infection. In this study, we aimed to assess the enduring impacts of COVID-19 on the vascular function of college students by conducting follow-up measurements a minimum of two months post-infection. To gain a comprehensive understanding of the recovery status of all participants two months after infection, we conducted a comparative analysis of their conditions before and after COVID-19. Furthermore, to explore the disparities in vascular endothelial recovery during the early versus late convalescent phases, we employed the median time post-infection as the threshold for stratifying the participants into distinct groups. This categorization allowed for a more precise investigation of the changes in vascular function over time post-infection. By meticulously comparing hemodynamic indicators, including endothelial function, arterial stiffness, and blood pressure, between the early recovery group and the late recovery group, we were able to delineate the temporal trajectory of vascular recovery following COVID-19.
Participants
All participants were college students. Inclusion criteria were as follows: (1) aged between 18 and 25 years, regardless of gender; (2) no prior history of COVID-19 infection before the COVID-19 restrictions were lifted in China, with a confirmed diagnosis of COVID-19 infection after December 2022 as well as a time interval of at least 2 months since infection; (3) no other physical or mental illnesses, and no significant history of surgical interventions; (4) no recent medication use within the past three months; (5) participants who had undergone cardiovascular testing in our laboratory before the COVID-19 infection.
Exclusion criteria were as follows: (1) smoking; (2) exercise regularly (3–5 times a week, about 30 min each time, for at least 6 weeks or more); (3) presence of heart disease or musculoskeletal disorders, and a history of major surgical interventions; (4) inability to comply with the trial protocol; (5) COVID-19 infection resulted in hospitalization.
A total of 37 participants were recruited for this study, which was approved by the Ethics Committee of Guangzhou Sport University (Protocol number: 2023LCLL-53). Before the beginning of the experiment, all participants were informed about the purpose of the study and signed written informed consent forms. The study protocol conforms to the ethical guidelines of the Declaration of Helsinki.
Study measurements
Endothelial function
The vascular endothelial function can be assessed using the non-invasive FMD measurement, which is associated with coronary artery endothelial function and independently predicts cardiovascular disease (CVD) outcomes [17]. Before the test, participants were instructed to rest in a quiet and temperature-controlled environment for 15 min. The FMD test was performed using a non-invasive ultrasound system (UNEXEF38G, UNEX, Nagoya, Japan) equipped with a high-resolution linear array transducer and edge tracking function [18, 19]. The participant was placed in a supine position, and the H-type transducer was utilized to capture the longitudinal view of the right brachial artery. The average value of the arterial diameter was recorded over a 10-heartbeat period at the end of diastole, establishing the baseline diameter for the artery. The probe was then kept in place, and a 5-minute ischemic occlusion was performed with a cuff inflated to a pressure 50 mmHg above the systolic blood pressure. The maximum diameter of the artery post-ischemic reactive hyperemia was documented from 30 s to 2 min following the release of the cuff. Taking into account the effects of shear stress, the probe was delicately positioned over the pulsatile site of the brachial artery, located 5–10 cm proximal to the right elbow joint of the participant (ensuring no heavy compression was applied to the brachial artery). Upon obtaining a complete and clear visualization of the intima-media complex, the probe was firmly fixed in place for the entire duration of the assessment. All testing was performed by an operator with substantial experience.The calculation formula is as follows: FMD (percentage) = ([peak diameter - baseline diameter]/baseline diameter) × 100 [20].
Arterial stiffness and blood pressure
Arterial stiffness was assessed using a PWV measurement device (BOSO ABI Systems 100, Bosch & Sohn, Germany) [21, 22]. Before the test, participants were instructed to lie flat and rest for 5 min with their hands and legs uncrossed. During the test, an experienced experimenter placed inflatable cuffs on the participant’s limbs as instructed. The variables included ankle-brachial index (ABI), carotid-femoral pulse wave velocity (cfPWV), brachial-ankle pulse wave velocity (baPWV), blood pressure (BP), and heart rate (HR) were measured. The ABI is a marker for assessing lower extremity arterial stenosis and peripheral arterial occlusive disease (PAOD) caused by atherosclerosis [23]. The two most commonly used methods for measuring PWV are cfPWV and baPWV, both of which can assess aortic and systemic arterial stiffness, respectively [24]. These two markers are considered simple and reliable indicators of conditions of central and systemic arterial function [25, 26]. The device can measure baPWV on both sides of the body, referred to as LbaPWV (left brachial-ankle pulse wave velocity) and RbaPWV (right brachial-ankle pulse wave velocity).
Sample size considerations
In this study, G*Power software (version 3.1.9.7) was used to determine the required sample size for our research investigation. We assumed a medium effect size of 0.50, a significance level of 0.05, and a desired power of 0.80 for sample size estimation. G*Power recommended a total sample size of 34 participants to achieve the desired power level. By using G*Power for sample size calculation, we ensured that our study had sufficient statistical power to detect meaningful effects. This information guided our recruitment process and helped assess the feasibility of our research objectives.
Data analysis
Initially, the normality of the data was assessed using the Shapiro-Wilk normality test. For data that followed a normal distribution, a paired t-test was conducted. For data that did not follow a normal distribution, a non-parametric test such as the Wilcoxon signed-rank test was employed. Descriptive statistics were computed for normally distributed data, including the mean and standard deviation, while for non-normally distributed data, the median and interquartile range were reported.
To evaluate the longitudinal changes in COVID-19 infected individuals during the complete timeline post-infection and to discern the differences in outcomes between the early and late stages of convalescence. The association between these changes (FMD, cfPWV, ABI, baPWV, HR, and BP) throughout the complete post-infection timeline and variables such as the time of COVID-19 infection, age, and body mass index (BMI) was analyzed using the Spearman correlation coefficient.
Furthermore, based on the results of the correlation analysis, a simple linear regression (SLR) analysis was conducted to explore the relationship between the time of COVID-19 infection and the changes of LbaPWV, RbaPWV, and diastolic blood pressure (DBP) before and after COVID-19 infection.
A significance level of p < 0.05 was considered to indicate statistical significance in the analysis. The statistical analysis was performed using Stata (version 12.0).
Results
A total of 37 participants were included in this pre-post-controlled study. Each participant visited the laboratory twice. The demographic and clinical characteristics of the participants are presented in Table 1. In our study, we meticulously analyzed the temporal aspects of health assessments related to COVID-19 infection. The median interval from infection onset to the second follow-up test was 114 days (IQR: 95 to 122 days). We also determined the mean time from the pre-COVID-19 assessment to the post-COVID-19 follow-up to be 188 days, with a relatively small standard deviation of 22 days, indicating consistency among participants. The range extended from 144 to 219 days, acknowledging some variability. This detailed analysis ensures a robust understanding of the temporal context and accounts for variability in our study outcomes.
The hemodynamic measurements results are presented in Tables 2 and 3.
Endothelial function
By conducting a Wilcoxon signed-rank test, we found a significant difference in FMD between pre- and post-COVID-19 infection (Z = − 3.20, p < 0.001). The median FMD after COVID-19 infection was 10.8%, with an IQR of 10.1–11.4%, while the median FMD before COVID-19 infection was 11.2%, with an IQR of 10.3–15.1%.
However, while stratified by the median time post-infection into early (n = 20) and late recovery (n = 17) groups, differences in FMD were noted. In the early recovery group, a significant difference in FMD was observed (p = 0.044), whereas the late recovery group showed no significant change (p = 0.290). Specifically, in the early recovery group, the median FMD prior to COVID-19 infection was 12.65%, with an IQR of 10.30–15.38%, which decreased to a median of 10.80% post-infection, with an IQR of 9.68–11.55%. In contrast, the late recovery group exhibited a median FMD of 11.00% before infection, with an IQR of 10.45–12.95%, and a median FMD of 11.10% after infection, with an IQR of 10.30–11.35%, indicating a trend towards stability in FMD values.
Arterial stiffness and blood pressure
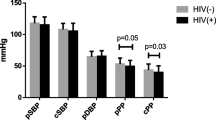
The study’s findings indicate that throughout the course of COVID-19 infection, there was a significant increase in cfPWV with a mean difference of 0.44 m/s (p = 0.022) and SBP with a mean difference of 3.24 mmHg (p = 0.047). DBP also exhibited an increase, though it was not statistically significant, with a mean difference of 2.65 mmHg (p = 0.068). No significant changes were observed in other arterial stiffness measures such as baPWV, ABI, and HR (p > 0.05).
Further analysis stratifying the recovery period by the median post-infection time revealed that in the early phase (n = 20), there were significant increases in LbaPWV and RbaPWV (p = 0.035 and p = 0.010, respectively). In contrast, during the late recovery phase (n = 17), DBP showed a significant increase (p = 0.008), whereas no significant changes were noted in the early phase (p > 0.05). Other indicators did not display significant differences across the recovery phases (p > 0.05).
Correlation and regression analysis
To investigate the effects of BMI, age, and the change in time since COVID-19 infection on endothelial vascular function and arterial stiffness, we conducted further correlation and regression analyses using the change values from pre- to post-infection. The results of Spearman correlation analysis, which incorporated these change values, showed strong negative correlations between the change in time since COVID-19 infection and the change in baPWV (p < 0.01), and a positive correlation with the change in DBP (p < 0.01). Additionally, a significant positive correlation was observed between the change in RABI and the change in LABI (p < 0.01). The change in LbaPWV and the change in RbaPWV exhibited a strong positive correlation (p < 0.01), while the change in SBP and the change in DBP showed a moderate positive correlation (p < 0.05). No significant correlations were found between BMI, age, and the changes in FMD, ABI, baPWV, cfPWV, HR, and BP (Table 4).To further investigate the impact of the time of COVID-19 infection on arterial stiffness, we conducted a linear regression analysis and illustrated the fitting effect using scatterplots. As shown in Figure 1, the time of COVID-19 infection had a significant negative effect on LbaPWV change (Fig. 1A), (regression coefficient: −0.045, p < 0.001, R2 = 0.38) and RbaPWV change (Fig. 1B), (regression coefficient: -0.042, p < 0.001, R2 = 0.32), explaining 38% and 32% of the variation in changes, respectively. Additionally, there was a significant positive effect on DBP change (Fig. 1C), (regression coefficient: 0.140, p = 0.024, R2 = 0.14 ), accounting for 14% of the variation.

The impact of the time of COVID-19 infection on LbaPWV, RbaPWV, and DBP. A: A reduction in LbaPWV with increasing time of COVID-19 infection was shown, as indicated by the SLR model with 95% confidence interval (CI) and fitting curve (R2 = 38%, p < 0.001). B: A reduction in RbaPWV with increasing time of COVID-19 infection was shown, as supported by the SLR model with 95% confidence interval (CI) and fitting curve (R2 = 32%, p < 0.001). C: An increase in DBP with increasing time of COVID-19 infection was shown, as depicted by the SLR model with 95% confidence interval (CI) and fitting curve (R2 = 14%, p = 0.024)
Discussion
The present study is the first pre-post-controlled study to examine the long-term effects of COVID-19 infection on vascular function in college students. The experimental results revealed that even mild COVID-19 infection in college students who did not require hospitalization resulted in significant changes in vascular function during 2 to 5 months post-infection. Our data indicated that endothelial dysfunction, increased arterial stiffness, and elevated blood pressure were the main manifestations of post-COVID-19 infection, which aligned with our hypothesis. Additionally, regression analysis demonstrated that as the time of COVID-19 infection increased, LbaPWV and RbaPWV decreased, suggesting a certain degree of improvement in arterial stiffness among young individuals over time. This is consistent with our stratification of the post-infection period into early and late recovery phases based on the median time of infection. During the early recovery phase, there was a significant increase in both LbaPWV and RbaPWV. In contrast, during the late recovery phase, these indicators showed no significant differences and tended to revert to levels prior to the COVID-19 infection. However, an unexpected outcome was observed for diastolic blood pressure (DBP), indicating a prolonged impact of COVID-19 on blood pressure levels. When we stratified the recovery period based on the median time since infection, we found no statistically significant difference in DBP during the early recovery phase. In contrast, the late recovery phase was characterized by a significant increase in DBP. This discrepancy may be attributed to the infection’s effects becoming more pronounced over time, with the late recovery group showing more evident impacts compared to the early recovery group, where the effects might not have had adequate time to manifest. Currently, possible mechanisms for cardiovascular damage in the long-term effects of COVID-19 infection include the direct impact of the SARS-CoV-2 virus on the myocardium, microthrombotic injury to blood vessels and endothelium, and persistent systemic inflammation [27]. Libby et al. suggested that COVID-19 is a disease that ultimately affects the endothelium [28]. The impact of SARS-CoV-2 on the endothelial layer can be attributed to the binding of its spike (S) protein to ACE2 on the host cell surface, which facilitates viral entry into the host cell and subsequently leads to a condition known as endotheliitis [29]. SARS-CoV-2 infection can also elicit systemic inflammation and cytokine release, impairing the bioavailability of nitric oxide (NO) and leading to dysregulation of vascular tone, ultimately resulting in arterial stiffness [8]. Our study found that within 2 to 5 months following COVID-19 infection, there was a significant decrease in FMD and an increase in cfPWV, indicating long-term negative effects on endothelial function and arterial stiffness. A prospective study compared vascular function among healthy individuals, individuals with a history of COVID-19 infection 4 months prior, and individuals with hypertension and reported that both the COVID-19 patients and hypertensive patients exhibited similar FMD values, which were lower than those of healthy individuals [9]. Furthermore, another study found that in previously hospitalized COVID-19 patients, endothelial function improved at 6-month follow-up but remained lower than that in healthy individuals [30]. The study suggested that even in individuals without any pre-existing cardiovascular diseases before COVID-19 infection, the risk of cardiovascular diseases remained elevated within 12 months of COVID-19 infection [31]. However, contrary research findings indicated that COVID-19 (Omicron variant) did not have any impact on the vascular and cardiac autonomic function in young individuals [10]. A possible reason for this finding may be the limited sample size, with only 23 participants infected with COVID-19, which may not adequately reflect the impact of COVID-19 on the cardiovascular system.
Multiple studies have demonstrated that BP levels increased following COVID-19 infection [32,33,34,35,36]. SARS-CoV-2 enters the human body by binding to ACE2, which typically converts Angiotensin I in the renin-angiotensin-aldosterone system (RAAS) to Angiotensin II, thus influencing BP [37]. During hospitalization, critically ill patients infected with SARS-CoV-2 exhibited a significant increase in BP [38]. A retrospective study involving 153 patients revealed an increase in SBP and DBP following SARS-CoV-2 infection. Furthermore, 18 cases developed new-onset hypertension within 30 days [33]. Wrona et al. suggested that the sequelae of COVID-19 include newly developed diabetes, hypertension, and dyslipidemia [39]. Our study found that SBP significantly increased after COVID-19 infection, with a borderline significant elevation in DBP. The possible reason is that COVID-19 infection leads to an inflammatory response, and during the inflammatory process, inflammatory mediators (such as cytokines) produced in the body may cause vasoconstriction and increase blood pressure.
It is noteworthy that our regression model, when analyzing the 2- to 5-month post-infection period, showed that as the time of COVID-19 infection increased, baPWV decreased, while DBP increased. This suggests that arterial stiffness improved with time after COVID-19 infection but the virus had long-term effects on BP. Although previous studies had indicated that patients with COVID-19 showed gradual improvement in endothelial function during the 6-month follow-up period after discharge, their endothelial function still lagged behind that of healthy individuals [40]. Another study demonstrated that at least 6 months after infection, COVID-19 survivors without other comorbidities associated with endothelial damage only showed mild evidence of endothelial dysfunction [41]. However, there were also studies indicating that the vascular damage became more severe with the progression of infection time [42]. Further investigation is warranted to explore the long-term effects of cardiovascular damage following COVID-19 infection.
In the present study, we did not observe a significant difference in the ABI index and HR between pre-post COVID-19 pandemic. Abnormal ABI values, defined as < 0.9 or > 1.3 m/s, are indicative of increased risk for overall mortality and cardiovascular mortality [43]. In our study, we observed no significant difference in the ankle-brachial index (ABI) values between the pre-infection and post-infection periods, regardless of whether the post-infection period was within the initial 2 to 5 months or stratified into early and late recovery phases based on the median time since infection. In all cases, the ABI values of all participants remained within the normal range. This may be attributed to the fact that our subjects consisted of young college students, and none of them were hospitalized due to COVID-19 infection. A recent study had indicated that SARS-CoV-2 induced vagal neuropathy, leading to autonomic dysfunction and potential long-term impairment of autonomic function [44]. Additionally, a study found that SARS-CoV-2 infection increased sympathetic nerve activation in young individuals, but had no significant effect on resting hemodynamics and speculated that the impact of COVID-19 on endothelial function and arterial stiffness may be more pronounced in older individuals [45]. Therefore, further investigation is warranted to identify the impact of COVID-19 on the autonomic nervous system, particularly its long-term effects.
Our study also has some limitations. Due to the retrospective nature of the pre-COVID-19 data, our sample size was limited, and further expansion was not possible. Additionally, the selection of young college students as the study population may affect the generalizability of the results. Furthermore, the duration between the pre- and post-measurements varied among participants.
In summary, our study indicates that even young college students with mild COVID-19 infections sustain significant adverse effects on endothelial function, arterial stiffness, and blood pressure within 2 to 5 months post-infection. Additionally, comparative data between early and late recovery phases, coupled with regression analyses across the entire timeframe, suggest that while vascular damage may diminish over time following COVID-19 infection, the elevation in blood pressure may endure for an extended period.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- FMD:
-
Flow-mediated dilation
- ABI:
-
Ankle-brachial index
- PWV:
-
Pulse wave velocity
- BaPWV:
-
Brachial-ankle pulse wave velocity
- LbaPWV:
-
Left brachial-ankle pulse wave velocity
- RbaPWV:
-
Right brachial-ankle pulse wave velocity
- cfPWV:
-
Carotid-femoral pulse wave velocity
- HR:
-
Heart rate
- BP:
-
Blood pressure
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- SARS-CoV-2:
-
Syndrome coronavirus 2
- COVID-19:
-
Coronavirus disease 2019
- ACE2:
-
Angiotensin-converting enzyme 2
- ESH:
-
European society of hypertension
- ESC:
-
European Society of cardiology
- CAD:
-
Coronary artery disease
- CHF:
-
Congestive heart failure
- CVD:
-
Cardiovascular disease
- PAOD:
-
Peripheral arterial occlusive disease
- NO:
-
Nitric oxide
- RAAS:
-
Renin-angiotensin-aldosterone system
References
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270–3.
World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2023 [cited 2023 July 26]. https://covid19.who.int/?gclid=CjwKCAiAsaOBBhA4EiwAo0_AnPoKZSzbiK7p4rGVggeX8BwZkkKOksOTzIDYbYExXTksUQC5aIC8lRoCxXgQAvD_BwE.
Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–31.
Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22(4):e102–7.
Abbasi J. The COVID Heart-One Year after SARS-CoV-2 infection, patients have an array of increased Cardiovascular risks. JAMA. 2022;327(12):1113–4.
Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–e808.
Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet (London England). 2020;395(10234):1417–8.
Schnaubelt S, Oppenauer J, Tihanyi D, Mueller M, Maldonado-Gonzalez E, Zejnilovic S, et al. Arterial stiffness in acute COVID-19 and potential associations with clinical outcome. J Intern Med. 2021;290(2):437–43.
Lambadiari V, Mitrakou A, Kountouri A, Thymis J, Katogiannis K, Korakas E, et al. Association of COVID-19 with impaired endothelial glycocalyx, vascular function and myocardial deformation 4 months after infection. Eur J Heart Fail. 2021;23(11):1916–26.
Skow RJ, Nandadeva D, Grotle AK, Stephens BY, Wright AN, Fadel PJ. Impact of breakthrough COVID-19 cases during the omicron wave on vascular health and cardiac autonomic function in young adults. Am J Physiol Heart Circ Physiol. 2022;323(1):H59–64.
Mansiroglu AK, Disikirik T, Seymen H, Cosgun M, Sincer I. Assessment of aortic stiffness by Transthoracic Echocardiographic in Young COVID-19 patients. J Cardiovasc Echography. 2022;32(1):23–8.
Boutouyrie P, Chowienczyk P, Humphrey JD, Mitchell GF. Arterial stiffness and Cardiovascular Risk in Hypertension. Circul Res. 2021;128(7):864–86.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25(6):1105–87.
Zhang Y, Agnoletti D, Protogerou AD, Topouchian J, Wang JG, Xu Y, et al. Characteristics of pulse wave velocity in elastic and muscular arteries: a mismatch beyond age. J Hypertens. 2013;31(3):554–9. discussion 9.
Jia G, Aroor AR, Jia C, Sowers JR. Endothelial cell senescence in aging-related vascular dysfunction. Biochim et Biophys acta Mol Basis Disease. 2019;1865(7):1802–9.
Siasos G, Zografos T, Oikonomou E, Papavassiliou AG, Stefanadis C, Tousoulis D. Flow-mediated dilation: is it just a research tool or a useful biomarker for cardiovascular prognosis. Int J Cardiol. 2015;180:154–7.
Thijssen DHJ, Bruno RM, van Mil A, Holder SM, Faita F, Greyling A, et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur Heart J. 2019;40(30):2534–47.
Tang S, Huang W, Wang S, Wu Y, Guo L, Huang J, et al. Effects of aquatic high-intensity interval training and moderate-intensity continuous training on central hemodynamic parameters, endothelial function and aerobic fitness in inactive adults. J Exerc Sci Fit. 2022;20(3):256–62.
Huang J, Wang S, Xu F, Wang D, Yin H, Lai Q, et al. Exercise training with dietary restriction enhances circulating irisin level associated with increasing endothelial progenitor cell number in obese adults: an intervention study. PeerJ. 2017;5:e3669.
Harris RA, Nishiyama SK, Wray DW, Richardson RS. Ultrasound assessment of flow-mediated dilation. Hypertens (Dallas Tex: 1979). 2010;55(5):1075–85.
Diehm N, Dick F, Czuprin C, Lawall H, Baumgartner I, Diehm C. Oscillometric measurement of ankle-brachial index in patients with suspected peripheral disease: comparison with doppler method. Swiss Med Wkly. 2009;139(25–26):357–63.
Cai L, Huang J, Gao D, Zeng S, Tang S, Chang Z, et al. Effects of mind-body practice on arterial stiffness, central hemodynamic parameters and cardiac autonomic function of college students. Complement Ther Clin Pract. 2021;45:101492.
Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, et al. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126(24):2890–909.
Lu Y, Zhu M, Bai B, Chi C, Yu S, Teliewubai J et al. Comparison of carotid-femoral and brachial-ankle pulse-Wave Velocity in Association with Target Organ damage in the Community-Dwelling Elderly Chinese: the Northern Shanghai Study. J Am Heart Association. 2017;6(2).
Huang J, Lai Q, Wang D, Yin H, Liao J, Wang S, et al. Effects of Exercise Training with Dietary Restriction on arterial stiffness, central hemodynamic parameters and cardiac autonomic function in obese adolescents. Diabetes Metabolic Syndrome Obesity: Targets Therapy. 2019;12:2157–63.
Hu M, Wang S, Wang D, Lai Q, Chen X, Duan S, et al. Combined moderate and high intensity exercise with dietary restriction improves cardiac autonomic function associated with a reduction in central and systemic arterial stiffness in obese adults: a clinical trial. PeerJ. 2017;5:e3900.
Gyöngyösi M, Alcaide P, Asselbergs FW, Brundel B, Camici GG, Martins PDC, et al. Long COVID and the cardiovascular system-elucidating causes and cellular mechanisms in order to develop targeted diagnostic and therapeutic strategies: a joint Scientific Statement of the ESC Working Groups on Cellular Biology of the Heart and Myocardial and Pericardial diseases. Cardiovascular Res. 2023;119(2):336–56.
Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease. Eur Heart J. 2020;41(32):3038–44.
Kumar N, Kumar S, Kumar A, Bhushan D, Kumar A, Kumar A, et al. The COSEVAST Study Outcome: evidence of COVID-19 severity proportionate to surge in arterial stiffness. Indian J Crit care Medicine: peer-reviewed Official Publication Indian Soc Crit Care Med. 2021;25(10):1113–9.
Oikonomou E, Souvaliotis N, Lampsas S, Siasos G, Poulakou G, Theofilis P, et al. Endothelial dysfunction in acute and long standing COVID-19: a prospective cohort study. Vascul Pharmacol. 2022;144:106975.
Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3):583–90.
Laffin LJ, Kaufman HW, Chen Z, Niles JK, Arellano AR, Bare LA, et al. Rise in blood pressure observed among US adults during the COVID-19 pandemic. Circulation. 2022;145(3):235–7.
Akpek M, Does. COVID-19 cause. Hypertension? Angiol. 2022;73(7):682–7.
De Lorenzo R, Conte C, Lanzani C, Benedetti F, Roveri L, Mazza MG, et al. Residual clinical damage after COVID-19: a retrospective and prospective observational cohort study. PLoS ONE. 2020;15(10):e0239570.
Gameil MA, Marzouk RE, Elsebaie AH, Rozaik SE. Long-term clinical and biochemical residue after COVID-19 recovery. Egypt Liver J. 2021;11(1):74.
Nesan G, Keerthana D, Yamini R, Jain T, Kumar D, Eashwer A, et al. 3-Month Symptom-based Ambidirectional follow-up study among recovered COVID-19 patients from a Tertiary Care Hospital using Telehealth in Chennai, India. Inquiry: J Med care Organ Provis Financing. 2021;58:469580211060165.
Nashiry A, Sarmin Sumi S, Islam S, Quinn JMW, Moni MA. Bioinformatics and system biology approach to identify the influences of COVID-19 on cardiovascular and hypertensive comorbidities. Brief Bioinform. 2021;22(2):1387–401.
Angeli F, Zappa M, Oliva FM, Spanevello A, Verdecchia P. Blood pressure increase during hospitalization for COVID-19. Eur J Intern Med. 2022;104:110–2.
Wrona M, Skrypnik D. New-Onset Diabetes Mellitus, Hypertension, Dyslipidaemia as Sequelae of COVID-19 infection-systematic review. Int J Environ Res Public Health. 2022;19(20).
Evans PC, Rainger GE, Mason JC, Guzik TJ, Osto E, Stamataki Z, et al. Endothelial dysfunction in COVID-19: a position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovascular Res. 2020;116(14):2177–84.
Kozłowski P, Śmiarowski M, Przyborska W, Zemlik K, Małecka-Giełdowska M, Leszczyńska A et al. Mild-to-moderate COVID-19 convalescents may present pro-longed Endothelium Injury. J Clin Med. 2022;11(21).
Podrug M, Koren P, Dražić Maras E, Podrug J, Čulić V, Perissiou M et al. Long-term adverse effects of mild COVID-19 disease on arterial stiffness, and systemic and central hemodynamics: a Pre-post Study. J Clin Med. 2023;12(6).
Visonà A, De Paoli A, Fedeli U, Tonello D, Zalunardo B, Zanatta N, et al. Abnormal ankle-brachial index (ABI) predicts primary and secondary cardiovascular risk and cancer mortality. Eur J Intern Med. 2020;77:79–85.
Woo MS, Shafiq M, Fitzek A, Dottermusch M, Altmeppen H, Mohammadi B, et al. Vagus nerve inflammation contributes to dysautonomia in COVID-19. Acta Neuropathol. 2023;146(3):387–94.
Stute NL, Stickford JL, Province VM, Augenreich MA, Ratchford SM, Stickford ASL. COVID-19 is getting on our nerves: sympathetic neural activity and haemodynamics in young adults recovering from SARS-CoV-2. J Physiol. 2021;599(18):4269–85.
Acknowledgements
We are grateful to all the participants who participated in this study.
Funding
This work was supported by the Guangdong Basic and Applied Basic Research Foundation (No.2023A1515012011), the Guangdong Scientific Research Platform and Projects for the Higher-educational Institution (2023ZDZX2033), the Scientific Research Project of Sports Bureau of Guangdong Province (GDSS2022N012), and the Macao Science and Technology Development Fund (002/2023/ALC).
Author information
Authors and Affiliations
Contributions
Conceptualization, J.W.P., W.H.G., P.L.L., and J.H.H.; methodology, J.W.P.; software, D.D.G.; validation, J.W.P., W.H.G. and P.L.L.; formal analysis, J.W.P.; investigation, L.L.; data curation, J.H.G., J.L.H. and Z.D.Y; writing—original draft preparation, J.W.P.; writing—review and editing, W.H.G. and P.L.L.; visualization, J.W.P. and S.W.; supervision, J.H.H.; project administration, S.W., J.H.H. and M.H.; funding acquisition, J.H.H. and M.H. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was conducted with the approval of the Ethics Committee of Guangzhou Sport University (Protocol number: 2023LCLL-53) and adhered to the ethical guidelines outlined in the 1975 Declaration of Helsinki. Prior to the commencement of the experiment, all participants received detailed information about the study’s objectives and provided their written informed consent.
Consent for publication
All participants involved in the study have provided their informed consent for the publication of the research results. This consent is in line with the ethical guidelines and ensures that any personal data or identifiable information will be appropriately anonymized to protect individual privacy. The participants understand that their contributions may be included in various forms within the publication, and they have the right to retract their consent at any time prior to the actual publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, J., Guo, W., Li, P. et al. Long-term effects of COVID-19 on endothelial function, arterial stiffness, and blood pressure in college students: a pre-post-controlled study. BMC Infect Dis 24, 742 (2024). https://doi.org/10.1186/s12879-024-09646-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09646-w