
Abstract
Background
The objective of this study was to explore the correlation between statin administration in the intensive care unit (ICU) setting and the in-hospital mortality risk of patients suffering from sepsis-induced coagulopathy (SIC).
Methods
Utilizing a retrospective cohort study design, this investigation collected data from the Medical Information Mart for Intensive Care (MIMIC)-IV spanning 2008 to 2019. The diagnosis of SIC was established based on a SIC score of 4 or above. Statin usage during the ICU period was extracted from the prescription records based on the keywords of statin medications. The primary endpoint analyzed was the in-hospital mortality within the ICU, characterized by any death occurring during the ICU admission.
Results
During the follow-up, which had a median duration of approximately 7.28 days, 18.19% of the 4,777 SIC patients died in the ICU. Statin was linked with a decrease in the risk of in-hospital mortality for SIC patients in the ICU [hazard ratio (HR): 0.73, 95% confidence interval (CI): 0.60–0.89, P = 0.002]. Relative to rosuvastatin, the use of atorvastatin (HR: 0.54, 95% CI: 0.34–0.85, P = 0.008) or simvastatin (HR: 0.55, 95% CI: 0.33–0.92, P = 0.024), as well as combinations of multiple statins (HR: 0.36, 95% CI: 0.15–0.86, P = 0.022), was associated with a reduction in ICU in-hospital mortality risk. Subgroup analysis also suggested that the use of atorvastatin, simvastatin, or a combination of statins had an advantage over rosuvastatin in reducing ICU in-hospital mortality in SIC patients older than 65 years of age or SIC patients with respiratory failure or cardiogenic shock (all P < 0.05).
Conclusion
The present study supports the potential benefits of statin use in mortality in SIC patients during ICU stays. The study encourages clinicians to consider the benefits of statins and supports the ongoing exploration of statins for enhanced outcomes in critical care settings.
Similar content being viewed by others


Background
Sepsis is a life-threatening systemic inflammatory response syndrome (SIRS) characterized by a dysregulated host response to infection, ultimately resulting in septic shock and multiple organ failure; it is a common condition in the intensive care unit (ICU) [1, 2]. Sepsis-induced coagulopathy (SIC) is a frequent complication of sepsis, characterized by the systemic activation of coagulation pathways, resulting in coagulation dysfunction associated with the condition [3]. The reported incidence of SIC was approximately 60% in patients with sepsis [4]. Compared to sepsis patients without SIC, individuals with SIC experience higher mortality rates and extended ICU hospital stays [3, 5]. Therefore, identifying effective treatment strategies to reduce mortality in patients with SIC is crucial for mitigating the overall disease burden.
HMG-CoA reductase inhibitors, commonly known as statins, are traditionally used to lower the level of blood cholesterol in patients with cardiovascular diseases or to prevent cardiovascular events [6]. In recent years, statins have gained attention for their immunomodulatory, anti-inflammatory, and antioxidant effects, being investigated as host-directed therapy for infectious disease [7, 8]. Vascular endothelial dysfunction serves as an ideal alternative therapeutic target for sepsis, as it precedes organ dysfunction and is involved in the pathophysiology of organ perfusion, vascular permeability, and the activation of coagulation cascade reactions [9, 10]. Statins have been observed to potentially influence coagulation function, with evidence suggesting their role in enhancing endothelial function [9, 11]. Additionally, research indicates that statins regulate various coagulation factors, leading to coagulation inhibition and increased fibrinolysis [12]. The use of statins has been reported to reduce the risk of thrombus formation in patients [13, 14]. Recent animal experiments indicate that simvastatin, in a rat model of endotoxemia, has the potential to prevent SIC, while also improving the prognosis of coagulopathy [15, 16]. Therefore, we hypothesize that the use of statins in the ICU is associated with a lower in-hospital mortality risk of SIC patients.
Therefore, this study aims to investigate the association between the use of statins in the ICU and the in-hospital mortality risk of SIC patients based on the large critical care database. Additionally, the study further analyzes the effects of different types of statins, providing evidence-based insights for the intervention and reduction of disease burden in SIC patients.
Methods
Study design and population
A retrospective cohort study design was employed. The data were sourced from the Medical Information Mart for Intensive Care (MIMIC)-IV database, accessible at https://mimic.mit.edu/docs/iv/. The period of study enrollment spanned from 2008 to 2019. The MIMIC database is a large, freely available database comprising de-identified health-related data associated with over forty thousand patients who stayed in critical care units of the Beth Israel Deaconess Medical Center in Boston, Massachusetts [17]. The MIMIC database includes information such as demographics, vital signs, laboratory tests, medications, and more. The data of MIMIC database is derived from various sources including bedside monitors, medical devices, and electronic medical records. The database encompasses patients from neonates to the elderly, providing a broad spectrum for research. Patient records were selected from the MIMIC-IV database for this study based on the following inclusion criteria: (1) diagnosis of SIC at the time of ICU admission, and (2) age of 18 years or older. Exclusion criteria were: (1) a stay in the ICU of less than 24 h, and (2) incomplete survival information. The study was performed according to the Declaration of Helsinki. The employment of the MIMIC database in this research was authorized by the review boards of both the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center. As a result, obtaining an additional ethical approval statement from Hangzhou Xixi Hospital Affiliated to Zhejiang Chinese Medical University was deemed unnecessary.
Data extraction
The data extracted from the database included the following: (1) baseline characteristics: age (years), gender (Male or Female), race (White, Asian, Black, Hispanic/Latino, Others, and Unknown), marital status (Married, Single/Divorced/Widowed, and Unknown), ICU type [coronary care unit (CCU), medical intensive care unit (MICU), surgical intensive care unit (SICU), and Others], and weight (kg); (2) comorbidities: acute kidney injury (AKI), respiratory failure, and cardiogenic shock; (3) vital signs: heart rate (bpm), systolic blood pressure (SBP, mmHg), diastolic blood pressure (DBP, mmHg), respiratory rate (insp/min), temperature (℃), and saturation of peripheral oxygen (SPO2, %); (4) scoring systems: Glasgow Coma Scale (GCS), Charlson comorbidity index (CCI), Sequential organ failure assessment (SOFA) score, simplified acute physiology score II (SAPSII), and SIRS; (5) laboratory parameters: white blood cell (WBC, K/uL) count, platelet count (K/uL), hemoglobin (g/dL), red cell distribution width (RDW, %), serum creatinine (Scr, mg/dL), estimated glomerular filtration rate calculated using the Chronic Kidney Disease Epidemiology Collaboration formula (eGFR-CKD-EPI, mL/min/1.73m2), international normalized ratio (INR), prothrombin time (PT, sec), partial thromboplastin time (PTT, sec), blood urea nitrogen (BUN, mg/dL), glucose (mg/dL), lactate (mmol/L), pH, sodium (mEq/L), potassium (mEq/L), chloride (mEq/L), bicarbonate (mEq/L), anion gap (mEq/L), and magnesium (mg/dL); (6) intervention: mechanical ventilation (yes or no), vasopressors (yes or no), midazolam (yes or no), propofol (yes or no), dexmedetomidine (yes or no), antibiotics (yes or no), platelet transfusion (yes or no), plasma transfusion (yes or no), vitamin K (yes or no), heparin (yes or no), statins use (yes or no), and type of statins (Rosuvastatin,
Atorvastatin, Pravastatin, Simvastatin, More than one, Others, and No).
Definitions and measurements
Sepsis was identified in accordance with the criteria outlined in Sepsis-3 [10]. Briefly, this involved patients who presented with a documented or suspected infection and experienced an acute increase of 2 points or more in their total SOFA score, which was indicative of sepsis. Patients initially diagnosed with sepsis were subsequently diagnosed with SIC if they presented with an SIC score of 4 or higher [18]. Statin usage during the ICU period was extracted from the prescription records based on the keyword of statin medications. The use of statins during the ICU period was oral.
AKI was determined based on the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. According to this definition, AKI was diagnosed in cases where there was an increase in Scr level by 0.3 mg/dl within a 48-hour period or an elevation in Scr to 1.5 times the baseline value, which was known or presumed to have occurred within the preceding 7 days, or a urine output of less than 0.5 mL/kg/h for a duration of 6 h [19]. Respiratory failure was identified using the International Classification of Diseases, Ninth Revision (ICD-9) codes 51,881, 51,883, and 51,884, and the first three characters of the Tenth Revision (ICD-10) as J96. Cardiogenic shock was classified using the ICD-9 code 78,551, and the first four characters of the ICD-10 as R570. The criteria for SIRS included: (1) tachycardia, defined as a heart rate exceeding 90 beats per minute, (2) tachypnea or hyperventilation, characterized by a respiratory rate greater than 20 breaths per minute or the partial pressure of carbon dioxide (PaCO2) below 32 mmHg, (3) fever or hypothermia, indicated by a body temperature higher than 38 °C or lower than 36 °C, and (4) leucocytosis, leukopenia, or bandemia, defined as a WBC count exceeding 12 × 109/L, falling below 4 × 109/L, or bandemia of 10% or more. SIRS status (range, 0 [best] to 4 [worst] criteria) [20].
Antibiotic usage was extracted based on the “antibiotics” category in the “input” database. eGFR_CKD-EPI (mL/min/1.73m2) = 141 × min(Scr/κ, 1)α × max(Scr/κ, 1) -1.209 × 0.993age × 1.018 (if female), where κ was 0.7 for females and 0.9 for males, α was − 0.329 for females and − 0.411 for males, “min” indicated the minimum of Scr/κ or 1, and “max” indicated the maximum of Scr/κ or 1. Scr was measured in mg/dL.
Outcome and follow-up
The outcome of this study was ICU in-hospital mortality, which was defined as any instance of death occurring within the hospital during the patient’s stay in the ICU. In-hospital data for the MIMIC-IV database were recorded by hospital departments. Follow-up was conducted during the patient’s hospitalization, with the endpoint being either in-hospital death or discharge. The median follow-up duration was 7.2799 (4.8771, 13.7597) days.
Statistical analysis
Quantitative data that follow a normal distribution were described using the mean ± standard deviation (Mean ± SD). For such data with homogeneity of variance, a T-test was used for pairwise comparisons between groups. When the data exhibited heterogeneity of variance, a Satterthwaite’s approximation T-test was employed for pairwise group comparisons. Quantitative data that did not conform to a normal distribution were described using the median and interquartile range (IQR). The Wilcoxon rank-sum test was utilized for comparing differences between groups for these data sets. For categorical data, the distribution was described using the number of cases and percentages [n (%)]. Differences between groups were assessed using the Chi-square test or Fisher’s exact test. Variables with a missing data rate exceeding 20% were excluded from the analysis. For variables with a missing data rate of 20% or less, multiple imputation was conducted to address the missing values. Sensitivity analyses were performed to compare the results before and after imputation to assess the impact of the imputation on the study findings.
Univariate Cox regression analysis was utilized to assess the association between all potential confounding variables (excluding those involved in calculating SAPSII, SOFA, CCI, GCS, SIRS, and anion gap, but retaining age) and the in-hospital mortality in SIC patients. Variables with a P-value less than 0.05 were selected for further analysis.
Subsequently, a Lasso regression model was constructed utilizing these variables. The selection of the optimal tuning parameter λ was based on the minimization of the squared error, corresponding to a standard deviation of prediction error. This process resulted in the retention of the following variables: age, type of ICU, AKI, respiratory failure, cardiogenic shock, pre-ICU statin use, SpO2, SAPS II, CCI, SIRS, RDW, PT, PTT, glucose, lactate, anion gap, use of vasopressors, midazolam, propofol, dexmedetomidine, type of antibiotics, vitamin K, and heparin. Variance Inflation Factor (VIF) is a statistical measure used to assess the degree of multicollinearity among independent variables (Supplementary Table 1). Subgroup analyses were conducted based on age, gender, comorbidities, severity of illness, and types of statins. Kaplan-Meier (KM) survival curve was used to estimate the survival probabilities over time in SIC patients across different treatment groups. The primary metrics for assessment were the hazard ratio (HR) and confidence interval (CI). The significance level was set at alpha = 0.05. Data extraction was conducted using PostgreSQL version 14.7. Data cleaning, imputation of missing values, covariate selection, regression analyses, and subgroup analyses were performed using R version 4.2.3.
Results
Population selection process and characteristics of included populations
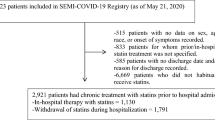
A total of 5,155 patients diagnosed as SIC upon ICU admission and aged ≥ 18 years from the MIMIC IV database were initially searched. After exclusions, the final sample count was 4,777. Figure 1 depicts the population selection process. Among 4,777 SIC patients, there were 869 (18.19%) patients who died during their ICU stay. In our analysis, we observed that 77.10% of the patients received statin therapy within the first 24 h of their hospital stay. The median duration of statin administration for the entire study population was 0.48 (0.33, 0.98) days (Supplementary Fig. 1). The median dosage of strains was 40 (20, 80) mg (Supplementary Fig. 2). The mean age was 65.54 ± 14.77 years. The gender distribution of the study population was composed of 35.59% females, amounting to 1,700 patients, and 64.41% males, totaling 3,077 patients. The ethnicity of the study’s participants was categorized as follows: White individuals constituted 2.37% of the population; Asians represented 6.57%; Blacks accounted for 3.41%; Hispanic or Latino individuals made up 4.27%; the category labeled as Other included 14.84%; and a significant portion, 68.54%, had an unspecified ethnicity, encompassing 3,274 patients. In the study, 51.58% of patients did not use any statin medications. Among those who used statins, 163 patients (3.41%) were prescribed rosuvastatin, while atorvastatin was used by 1,282 patients, representing 26.84% of the total. Pravastatin was the chosen medication for 191 patients, making up 4.00%, and simvastatin was used by 576 patients, accounting for 12.06%. A smaller proportion, 1.95% or 93 patients were treated with more than one type of statin, and another 8 patients, which was 0.16% of the sample, were categorized under “Others” for their statin type. There were significant differences between SIC patients with and without in-hospital mortality in age, gender, race, marital status, ICU type, pathogen, AKI, respiratory failure, cardiogenic shock, heart rate, hematological diseases, SBP, respiratory rate, SPO2, SAPS II, SOFA, GCS, CCI, SIRS, WBC, platelet count, RDW, Scr, eGFR-CKD-EPI, INR, PT, PTT, BUN, glucose, lactate, pH, sodium, chloride, bicarbonate, anion gap, magnesium, statins use before ICU admission, type of antibiotics, mechanical ventilation, vasopressors, midazolam, propofol, dexmedetomidine, antibiotics, platelet transfusion, plasma transfusion, Vitamin K, heparin, statins use, and type of statins. Table 1 summarizes the characteristics of the included populations.

The population selection process. SIC, sepsis-induced coagulopathy; ICU, intensive care unit; MIMIC, Medical Information Mart for Intensive Care
Association between statin use and the risk of in-hospital mortality in patients with SIC
The association between statin use and the risk of in-hospital mortality in patients with SIC is presented in Table 2. The result indicated that the use of statins was associated with a lower risk of in-hospital mortality in the ICU among patients with SIC (HR: 0.73, 95% CI: 0.60–0.86, P = 0.002).
Association between different types of statins and the risk of in-hospital mortality in patients with SIC
When using rosuvastatin as a reference, the administration of atorvastatin (HR: 0.54, 95% CI: 0.34–0.85, P = 0.008), simvastatin (HR: 0.55, 95% CI: 0.33–0.92, P = 0.024), or a regimen combining multiple statins (HR: 0.36, 95% CI: 0.15–0.86, P = 0.022) was correlated with a reduced risk of in-hospital mortality among patients suffering from SIC. Table 3 shows the association between different types of statins and the risk of in-hospital mortality in patients with SIC. The KM curve shows that SIC patients who received statins had better survival probabilities compared to those who did not receive any statins, with the group receiving more than one statin showing the highest survival probability (Fig. 2).

The survival probabilities over time in SIC patients across different treatment groups. SIC, sepsis-induced coagulopathy
Subgroup analysis of the association between statin use and in-hospital mortality risk in patients with SIC
Table 4 suggests an association between statin use and a lower risk of in-hospital mortality in patients with SIC aged < 65 years (HR: 0.54, 95% CI: 0.36–0.81, P = 0.003), regardless gender (male or female), in patients with respiratory failure (HR: 0.77, 95% CI: 0.60–0.98, P = 0.034), in patients without cardiogenic shock (HR: 0.71, 95% CI: 0.56–0.89, P = 0.003), and irrespective of the SIRS score being ≤ 1 or > 1.
Table 5 displays the subgroup analysis of the association between different types of statin medications and the risk of in-hospital mortality among various patients with SIC. For patients aged 65 and older, using rosuvastatin as a reference, there was an association between the use of atorvastatin (HR: 0.51, 95% CI: 0.31–0.83, P = 0.007), simvastatin (HR: 0.51, 95% CI: 0.29–0.88, P = 0.016), and the use of more than one statin (HR: 0.31, 95% CI: 0.11–0.85, P = 0.023) with a lower risk of in-hospital mortality in those with SIC. For females, using rosuvastatin as a reference, the associations between the use of atorvastatin, and the use of more than one statin with a lower risk of in-hospital mortality in patients with SIC were statistical significance. For patients with respiratory failure, using rosuvastatin as a reference, there was an association between the use of atorvastatin (HR: 0.36, 95% CI: 0.20–0.64, P = 0.001), simvastatin (HR: 0.43, 95% CI: 0.21–0.85, P = 0.016), and the use of more than one statin (HR: 0.16, 95% CI: 0.04–0.58, P = 0.005) with a lower risk of in-hospital mortality in those with SIC. As for patients with cardiogenic shock, when compared to rosuvastatin, the employment of atorvastatin, simvastatin or a regimen involving multiple statins was linked to a reduced in-hospital mortality risk among those diagnosed with SIC. In patients who had a SIRS score of 1 or less, compared to rosuvastatin as a baseline, the application of atorvastatin (HR: 0.38, 95% CI: 0.18–0.81, P = 0.013) was linked to a decreased risk of dying in the hospital among those suffering from SIC.
Discussion
In this cohort study, we used data from the MIMIC database to evaluate the association between the use of statins in the ICU and the in-hospital mortality risk of SIC patients. Our results demonstrated that the use of statins was associated with a lower risk of in-hospital mortality in the ICU among patients with SIC. When rosuvastatin served as a comparison, the utilization of atorvastatin or simvastatin, and more than one statin demonstrated a significant correlation with lower in-hospital mortality risk in SIC patients. According to the subgroup analyses, among patients with SIC who were 65 years or older or had respiratory failure or cardiogenic shock, the use of atorvastatin, simvastatin, or a combination of various statins was associated with a lower risk of in-hospital mortality compared to rosuvastatin.
Statins have been reported to be associated with lower mortality in patients with several diseases. In an umbrella review of meta-analyses, the protective effect of statins on infection-related mortality was observed [21]. In a study that included adults with non-dialysis advanced chronic kidney disease, statin users had lower infection-related mortality than non-users [22]. In a meta-analysis to investigate the effect of statins on COVID-19 outcomes, improved mortality in the COVID-19 ICU after statin therapy was observed [23]. In a single-center cohort study of 1179 patients, statin therapy during hospitalization for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection was associated with reduced short-term mortality [24]. Atorvastatin add-on therapy in patients with severe COVID-19 was associated with lower in-hospital mortality [25]. The benefit of statins in critically ill patients has also been suggested. The study by Harbi et al. [26], demonstrated that statin therapy during ICU admission was associated with lower hospital mortality. In a cohort study, acute respiratory distress syndrome (ARDS) patients who used statins before ICU admission experienced a 39% reduction in 30-day mortality and 38% reduction in 90-day mortality [27]. In a study on 1,315 patients with acute myocardial infarction (AMI) and diabetes, statins could significantly reduce ICU in-hospital mortality rates in patients [28]. The study by Chinaeke et al. [29], showed that patients in ICU with sepsis who had pre-ICU statin use had decreased mortality. This study found an association between statins and a lower risk of in-hospital mortality in the ICU among patients with SIC, illustrating the beneficial effect of statins during ICU in SIC patients.
The association between statin use and reduced in-hospital mortality risk in patients with SIC may be attributed to several mechanisms. Firstly, statins have been found to have anti-inflammatory properties [30, 31]. In the context of sepsis, statins may modulate the body’s immune response, reducing systemic inflammation and potentially preventing the progression to severe condition of sepsis [32]. Secondly, statins enhance endothelial function by increasing the bioavailability of nitric oxide [33]. The improvement in endothelial function may help maintain microvascular integrity in sepsis patients, reducing the risk of organ dysfunction [34]. Thirdly, SIC is characterized by a hypercoagulable state leading to microthrombi formation and impaired microcirculation [3]. Statins have been shown to exert antithrombotic effects by downregulating procoagulant factors and upregulating anticoagulant pathways, thereby helping to maintain a balance in coagulation [35]. Fourthly, beyond lipid-lowering and anti-inflammatory effects, statins possess immunomodulatory properties [36], potentially leading to a more balanced immune response during sepsis, which is critical for preventing excessive tissue damage. These mechanisms collectively contribute to the potential benefits of statin therapy in reducing the mortality risk in patients SIC during ICU. However, it’s important to note that while these mechanisms are supported by preclinical and observational studies, the effectiveness and safety of statin therapy in SIC require further validation.
In this study, when compared with rosuvastatin, the use of atorvastatin, simvastatin, or a combination of statins was significantly associated with a reduced risk of ICU in-hospital mortality among patients with SIC. A large propensity score-matched study of mortality in sepsis reported that simvastatin and atorvastatin were protective, while rosuvastatin was not [37]. In a retrospective analysis of patients selected from an institutional database of patients hospitalized with sepsis, pre-hospital atorvastatin use was associated with improved in-hospital mortality in septic patients when compared with pre-hospital simvastatin [38]. In the study by Brunetti et al. [39], atorvastatin in combination with rosuvastatin had lower cardiovascular mortality than simvastatin. This result may be attributed to the fact that different statins have different properties, including pharmacokinetics, dose ranges, and potential drug interactions [40, 41]. Our findings suggest that physicians need to consider which drug is more appropriate for SIC during ICU and whether a combination therapy is needed. Subgroup analysis also suggests that the use of atorvastatin, simvastatin, or a combination of statins may have an advantage over rosuvastatin in reducing ICU in-hospital mortality in SIC patients older than 65 years of age or with respiratory failure or cardiogenic shock. Our findings suggest that physicians should tailor individualized treatment plans based on the specific circumstances of patients. The personalized approach may ensure that patients receive the most appropriate treatment for their unique needs while minimizing potential risks.
Our research findings suggest that the use of statins is associated with a reduced risk of in-hospital mortality in patients with SIC, potentially offering a novel therapeutic strategy for clinicians. In managing patients with SIC, physicians could consider incorporating statins into the treatment regimen to enhance survival prospects. SIC typically presents with severe coagulation abnormalities, potentially leading to significant bleeding and thrombotic complications that are life-threatening. If statins can lower the risk of in-hospital mortality among these patients, this could contribute to improved patient quality of life, reducing unnecessary suffering and complications arising from the condition. Conducting subgroup analyses may further elucidate which specific patient subgroups are most likely to benefit from statin use. The subgroup analysis facilitates personalized treatment, ensuring that statins are utilized primarily for patients most likely to derive benefit, thereby minimizing unnecessary drug exposure and adverse effects. Our study may also prompt further research to explore the therapeutic role of statins in patients with SIC more deeply.
We must acknowledge the limitations of our study. Firstly, our research is a single-center retrospective cohort study. Single-center retrospective cohort studies inherently possess several limitations that can affect the generalizability and interpretability of their findings. These limitations include restricted generalizability due to data being collected from a single location, potential selection bias from the retrospective nature of data collection, information bias due to inaccuracies or incompleteness in medical records, and the inability to establish causal relationships between variables. Additionally, confounding variables, whether identified and controlled for or not, can obscure the true relationships being studied. Secondly, our study pertains to the analysis of statin combination therapy within the context of sepsis treatment. Due to constraints in the available dataset, we could not provide a detailed account of the specific statin combinations employed, the timing of their introduction, and the rationale behind their prescription. The database limitations resulted in a limited sample size for patients who received combination therapy, which restricted our ability to conduct a comprehensive analysis of this aspect of treatment. Thirdly, the protocols of statins remain unclear. The exact timing of statin administration and the criteria for dose determination were not detailed in the database, which could introduce potential biases in our analysis. We could not discern whether the statin doses were adjusted based on individual patient responses or other clinical parameters, which may have influenced the outcomes observed. Additionally, the absence of detailed protocols prevents us from fully elucidating the relationship between statin administration practices and patient outcomes. Fourthly, due to the limited data from the database, the comparative advantages and disadvantages of different statins were not explored. Our study highlights the need for future studies to specifically address the comparative effectiveness and safety of different statins and their dosages on mortality during IUC in SIC patients.
Conclusion
Our results indicate that the use of statins is associated with a reduced risk of in-hospital mortality among patients with SIC. Compared to rosuvastatin, the use of atorvastatin, simvastatin, or a combination of different statins may offer greater survival benefits for SIC patients in the ICU, particularly in those aged ≥ 65 and those with respiratory failure or cardiogenic shock. This finding underscores the potential clinical significance of selecting specific statins or their combinations to enhance survival outcomes for critically ill SIC patients.
Data availability
The datasets used and/or analyzed during the current study are available from the MIMIC-IV database, https://mimic.mit.edu/docs/iv/.
References
Srzić I, Nesek Adam V, Tunjić Pejak D. SEPSIS DEFINITION: WHAT’S NEW IN THE TREATMENT GUIDELINES. Acta Clin Croat. 2022;61(Suppl 1):67–72.
Markwart R, Saito H, Harder T, Tomczyk S, Cassini A, Fleischmann-Struzek C, Reichert F, Eckmanns T, Allegranzi B. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536–51.
Li Y, Li H, Wang Y, Guo J, Zhang D. Potential biomarkers for early diagnosis, evaluation, and prognosis of Sepsis-Induced Coagulopathy. Clin Appl thrombosis/hemostasis: Official J Int Acad Clin Appl Thrombosis/Hemostasis. 2023;29:10760296231195089.
Iba T, Levi M, Thachil J, Helms J, Scarlatescu E, Levy JH. Communication from the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis on sepsis-induced coagulopathy in the management of sepsis. J Thromb Haemost. 2023;21(1):145–53.
Lu Z, Zhang J, Hong J, Wu J, Liu Y, Xiao W, Hua T, Yang M. Development of a Nomogram to predict 28-Day mortality of patients with Sepsis-Induced Coagulopathy: an analysis of the MIMIC-III database. Front Med. 2021;8:661710.
Kulkarni S, Watts MM, Kostapanos M. Statins Bmj. 2024;384:e072584.
Parihar SP, Guler R, Brombacher F. Statins: a viable candidate for host-directed therapy against infectious diseases. Nat Rev Immunol. 2019;19(2):104–17.
Zhang K, Liu W, Liang H. Effect of statins on sepsis and inflammatory factors: a mendelian randomization study. Eur J Clin Invest 2024:e14164.
Yan J, Li S, Li S. The role of the liver in sepsis. Int Rev Immunol. 2014;33(6):498–510.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, et al. The Third International Consensus definitions for Sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–10.
Reriani MK, Dunlay SM, Gupta B, West CP, Rihal CS, Lerman LO, Lerman A. Effects of statins on coronary and peripheral endothelial function in humans: a systematic review and meta-analysis of randomized controlled trials. Eur J Cardiovasc Prev Rehabilitation. 2011;18(5):704–16.
Bianconi V, Sahebkar A, Banach M, Pirro M. Statins, haemostatic factors and thrombotic risk. Curr Opin Cardiol. 2017;32(4):460–6.
Kwon OC, Park YB, Park MC. Effect of statins on the prevention of recurrent thrombosis in thrombotic antiphospholipid syndrome. Rheumatology (Oxford). 2022;61(4):1548–55.
Rodriguez AL, Wojcik BM, Wrobleski SK, Myers DD Jr., Wakefield TW, Diaz JA. Statins, inflammation and deep vein thrombosis: a systematic review. J Thromb Thrombolysis. 2012;33(4):371–82.
La Mura V, Gagliano N, Arnaboldi F, Sartori P, Procacci P, Denti L, Liguori E, Bitto N, Ristagno G, Latini R et al. Simvastatin Prevents Liver Microthrombosis and Sepsis Induced Coagulopathy in a Rat Model of Endotoxemia. Cells : 2022, 11(7).
Xu M, Luo LL, Du MY, Tang L, Zhou J, Hu Y, Mei H. Simvastatin improves outcomes of endotoxin-induced Coagulopathy by regulating Intestinal Microenvironment. Curr Med Sci. 2022;42(1):26–38.
Johnson AEW, Bulgarelli L, Shen L, Gayles A, Shammout A, Horng S, Pollard TJ, Hao S, Moody B, Gow B, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1.
Iba T, Nisio MD, Levy JH, Kitamura N, Thachil J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: a retrospective analysis of a nationwide survey. BMJ Open. 2017;7(9):e017046.
Wang B, Li D, Cheng B, Ying B, Gong Y. The Neutrophil Percentage-to-Albumin Ratio Is Associated with All-Cause Mortality in Critically Ill Patients with Acute Kidney Injury. Biomed Res Int 2020, 2020:5687672.
Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, Bellomo R, Pilcher DV. Prognostic accuracy of the SOFA score, SIRS Criteria, and qSOFA score for In-Hospital mortality among adults with suspected infection admitted to the Intensive Care Unit. JAMA. 2017;317(3):290–300.
Ghayda RA, Han CH, Lee KH, Kim JS, Kim SE, Hong SH, Kim M, Kronbichler A, Tizaoui K, Li H, et al. The effect of statins on mortality among patients with infection: umbrella review of meta-analyses. Eur Rev Med Pharmacol Sci. 2021;25(6):2685–95.
Hsiao CC, Yeh JK, Li YR, Sun WC, Fan PY, Yen CL, Chen JS, Lin C, Chen KH. Statin uses in adults with non-dialysis advanced chronic kidney disease: focus on clinical outcomes of infectious and cardiovascular diseases. Front Pharmacol. 2022;13:996237.
Vahedian-Azimi A, Mohammadi SM, Heidari Beni F, Banach M, Guest PC, Jamialahmadi T, Sahebkar A. Improved COVID-19 ICU admission and mortality outcomes following treatment with statins: a systematic review and meta-analysis. Arch Med Sci. 2021;17(3):579–95.
Memel ZN, Lee JJ, Foulkes AS, Chung RT, Thaweethai T, Bloom PP. Statins are Associated with Improved 28-day mortality in patients hospitalized with SARS-CoV-2 infection. medRxiv; 2021.
Haji Aghajani M, Moradi O, Azhdari Tehrani H, Amini H, Pourheidar E, Hatami F, Rabiei MM, Sistanizad M. Promising effects of atorvastatin on mortality and need for mechanical ventilation in patients with severe COVID-19; a retrospective cohort study. Int J Clin Pract. 2021;75(9):e14434.
Al Harbi SA, Tamim HM, Arabi YM. Association between statin therapy and outcomes in critically ill patients: a nested cohort study. BMC Clin Pharmacol. 2011;11:12.
Mao H, Yu Y, Wang Q, Li H. Association between pre-ICU statin use and ARDS mortality in the MIMIC-IV database: a cohort study. Front Med. 2023;10:1328636.
Lu X, Zhang L, Li S, He D, Huang T, Lin H, Yin H, Lyu J. Association between statin use and the prognosis of patients with acute myocardial infarction complicated with diabetes. Front Cardiovasc Med. 2022;9:976656.
Chinaeke EE, Love BL, Magagnoli J, Yunusa I, Reeder G. The impact of statin use prior to intensive care unit admission on critically ill patients with sepsis. Pharmacotherapy. 2021;41(2):162–71.
Koushki K, Shahbaz SK, Mashayekhi K, Sadeghi M, Zayeri ZD, Taba MY, Banach M, Al-Rasadi K, Johnston TP, Sahebkar A. Anti-inflammatory action of statins in Cardiovascular Disease: the role of Inflammasome and Toll-Like receptor pathways. Clin Rev Allergy Immunol. 2021;60(2):175–99.
Weitz-Schmidt G. Statins as anti-inflammatory agents. Trends Pharmacol Sci. 2002;23(10):482–6.
Kouroumichakis I, Papanas N, Proikaki S, Zarogoulidis P, Maltezos E. Statins in prevention and treatment of severe sepsis and septic shock. Eur J Intern Med. 2011;22(2):125–33.
Chen WH, Chen CH, Hsu MC, Chang RW, Wang CH, Lee TS. Advances in the molecular mechanisms of statins in regulating endothelial nitric oxide bioavailability: interlocking biology between eNOS activity and L-arginine metabolism. Biomed Pharmacother. 2024;171:116192.
Joffre J, Hellman J, Ince C, Ait-Oufella H. Endothelial responses in Sepsis. Am J Respir Crit Care Med. 2020;202(3):361–70.
Owens AP 3rd, Mackman N. The antithrombotic effects of statins. Annu Rev Med. 2014;65:433–45.
Blanco-Colio LM, Tuñón J, Martín-Ventura JL, Egido J. Anti-inflammatory and immunomodulatory effects of statins. Kidney Int. 2003;63(1):12–23.
Lee CC, Lee MG, Hsu TC, Porta L, Chang SS, Yo CH, Tsai KC, Lee M. A Population-based Cohort Study on the drug-specific effect of statins on Sepsis Outcome. Chest. 2018;153(4):805–15.
Ouellette DR, Moscoso EE, Corrales JP, Peters M. Sepsis outcomes in patients receiving statins prior to hospitalization for sepsis: comparison of in-hospital mortality rates between patients who received atorvastatin and those who received simvastatin. Ann Intensive Care. 2015;5:9.
Brunetti ND, Correale M, Totaro A, Ferraretti A, Monaco I, Passero T, De Gennaro L, Di Biase M. Lower cardiovascular mortality with atorvastatin and rosuvastatin vs simvastatin: data from moderate-intensity statin users in an observational registry on chronic heart failure (Daunia Heart failure Registry). Int J Cardiol. 2015;194:23–7.
Hirota T, Fujita Y, Ieiri I. An updated review of pharmacokinetic drug interactions and pharmacogenetics of statins. Expert Opin Drug Metab Toxicol. 2020;16(9):809–22.
Lucía C-C, José L-C. Pharmacokinetic Aspects of Statins. In: Cardiovascular Risk Factors in Pathology. edn. Edited by Alaeddin A, Maria S, Minodora A. Rijeka: IntechOpen; 2020: Ch. 6.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YY and SZ designed the study. YY wrote the manuscript. XZ, MW, FZ, CL, and XL collected, analyzed, and interpreted the data. SZ critically reviewed, edited, and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

{kind=link}
Cite this article
Yao, Y., Zhao, X., Wang, M. et al. Association between the use of statins and in-hospital mortality risk in patients with sepsis-induced coagulopathy during ICU stays: a study based on medical information mart for intensive care database. BMC Infect Dis 24, 738 (2024). https://doi.org/10.1186/s12879-024-09636-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09636-y