
Abstract
Background
Carbapenem-resistant Pseudomonas aeruginosa (CRPA) infection has become a major public health concern. The recommendations for monotherapy and combination therapy in the current guidelines lack sufficient evidence to support them. The primary objective of this study is to determine the effectiveness of anti-Infective combination therapy compared to monotherapy in achieving clinical success in patients with CRPA infection and risk factors of clinical failure of monotherapy.
Methods
A retrospective study from Medical Information Mart for Intensive Care IV (MIMIC-IV) was conducted. We included adults with infections caused by CRPA. The outcomes of this study were clinical success, complete clinical success, and 28-day all-cause mortality.
Results
A total of 279 subjects were finally enrolled. The rate of clinical success for combination therapy was higher than that for monotherapy (73.1% versus 60.4%, p=0.028). Compared to clinical failure patients, patients in the clinical success group were more likely to die within 28 days after CRPA was found (48.3% versus 3.6%, p<0.001). In a multivariate logistic regression analysis, monotherapy was found to be significantly correlated with clinical success (OR, 0.559, 95% CI, 0.321-0.976; p = 0.041).
Conclusion
Combination therapy is more effective for CRPA infection patients, especially those whose SOFA score is ≥ 2 or whose Charlson comorbidity index is ≥ 6.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pseudomonas aeruginosa (P. aeruginosa) is a ubiquitous microorganism that causes different types of infections, primarily in immunosuppressed patients, critical care patients, or those with comorbidities [1]. P. aeruginosa is also one of the most common pathogens that causes nosocomial infections, including central line-associated bloodstream infections, ventilation-associated pneumonia [1].
For clinicians, selecting an appropriate antibiotic regimen for Carbapenem-resistant P. aeruginosa (CRPA) infections is a global challenge. Instead of carbapenems, other antibiotics, such as ceftolozane-tazobactam, aminoglycoside, and fosfomycin, can be used against CRPA [2, 3]. The rationale for combination anti-infective therapy against CRPA is based on the possibility of achieving a higher rate of bacterial killing. Current clinical guidelines suggest using combination therapy to treat patients with severe CRPA infections [2, 3]. However, it is a conditional recommendation for use, and insufficient evidence is available for this recommendation. Current guidelines do not provide a specific method to identify severe CRPA infections [2, 3]. Additionally, recent studies have demonstrated that the effects of monotherapy and combination therapy on the prognosis of CRPA infection remain controversial [4,5,6,7].
Furthermore, there is growing evidence of harm caused to individual patients by unnecessary antimicrobial use. More antibiotic use risks higher costs, and it is more likely to cause drug-related adverse events such as allergic or hypersensitivity reactions and kidney injury [8]. In addition to adverse drug reactions and drug toxicity, antimicrobial resistance is one of the most widely recognized mechanisms of antimicrobial-associated harm [8]. A prospective observational study found that concomitant use of several antimicrobials is associated with an excess mortality risk compared to monotherapy [9].
Sepsis is characterized by fatal organ dysfunction caused by an overwhelming host response to an infection. The sequential organ failure assessment (SOFA) score is predominantly used to assess the severity of organ dysfunction and the severity of septic shock in sepsis [10, 11]. The primary objective of this study is to determine the effectiveness of anti-Infective combination therapy compared to monotherapy in achieving clinical success in patients with CRPA infection and risk factors of clinical failure of monotherapy.
Methods
Study design
We conducted a retrospective cohort study from Medical Information Mart for Intensive Care IV (MIMIC-IV). MIMIC-IV is a database that included more than 2 million anonymized patients who were admitted to the critical care units of Beth Israel Deaconess Medical Center (BIDMC) from 2008 to 2019.
Database
This study utilized data from MIMIC-IV. Clinical variables such as demographics, comorbid diseases, laboratory tests, microbial test results, and antibiotic records were documented in this database. The study authors have already completed the training course to gain access to the database.
Study population
The inclusion criteria were (1) age ≥18 years at admission and (2) infection caused by CRPA. The exclusion criteria were as follows: 1) length of stay shorter than 3 days, 2) missing information about CRPA, and 3) no antibiotic against CRPA or duration of antibiotics against CRPA shorter than 3 days. To avoid the potential impact of previous antibiotic use, we also excluded patients who had received monotherapy with different types of antibiotics.
Data extraction
The Structured Query Language (SQL) with the PostgreSQL tool (version 9.6) was used to extract data from MIMIC-IV. The extracted data included demographics, SOFA scores, complete antibiotic records 10 days after CRPA was found, and laboratory tests. We also extracted the comorbidities, including hypertension, diabetes, myocardial infarction, chronic pulmonary disease, renal failure, cerebrovascular disease, and severe liver disease.
Definition
Clinical success events were as follows: 1). Correction of septic shock (systolic blood pressure >90 mm Hg without the need for vasopressor support); 2). Ventilation withdrawal for patients with pneumonia; 3), microbiological cure for patients with bacteremia (no growth in the blood of an index isolate on day 14 or before); and 4) improved or stable SOFA score (for baseline SOFA ≥3, we required that the score improve by at least 30%, and for a baseline SOFA < 3, we required that the score remain the same or decrease). Clinical failure events were as follows: 1). new septic shock (systolic blood pressure <90 mm Hg with vasopressor therapy); 2) new ventilation for patients with pneumonia; 3) new bacteremia; and 4) increased SOFA score (for SOFA ≥3, we required that the score increase more than 30%, and for baseline SOFA < 3, we required that the score be greater than 3).
Similar to a previous study [12], clinical success was defined as a composite of patient survival, at least one clinical success event, and no clinical failure events 14 days after CRPA was found. Complete clinical success was defined as a composite of patient survival and all clinical success events 14 after days CRPA was found. Patients who did not meet the clinical success criteria were classified as having clinical failure. The outcomes of this study were clinical success, complete clinical success, and 28-day all-cause mortality.
Statistical analysis
Continuous variables are described as the means and standard deviations and were compared pairwise with Student's t test and one-way ANOVA across groups. Categorical variables are presented as numbers and percentages and were compared using Pearson’s chi-square test or Fisher’s exact test as appropriate. We performed a survival analysis using the log-rank test and 28-day Kaplan-Meier curves. Univariate and multivariate analyses for assessing independent risk predictors were performed using the logistic regression model. All statistical analyses were performed using SPSS software (v23.0; IBM, Armonk, NY); a two-sided P<0.05 was considered statistically significant.
Results
Characteristics of different antibiotic regimens and outcomes patients
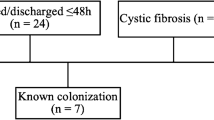
As shown in Fig. 1 (Title: Flow diagram for patient recruitment from the Multiparameter Intelligent Monitoring in Intensive Care IV database, Legends: This figure presented the patient recruitment process. Inclusion criteria in this study: 1. Age ≥ 18 years at admission. 2. Infection caused by Carbapenem-Resistant Pseudomonas aeruginosa (CRPA). Exclusion criteria in this study: 1. Length of stay shorter than 3 days. 2. Missing information about CRPA. 3. No antibiotic treatment against CRPA or duration of antibiotics against CRPA shorter than 3 days.4. Patients who received monotherapy with different types of antibiotics were also excluded to avoid potential impact of previous antibiotic use. Final sample: 279 patients meeting all inclusion criteria and not falling into any of the exclusion criteria were included in the final study sample.), a total of 279 subjects were enrolled for our final data analysis after screening by the inclusion and exclusion criteria. We excluded 110 patients based on various excluded criteria above.

Flow diagram for patient recruitment from the Multiparameter Intelligent Monitoring in Intensive Care IV database
Table 1 shows the characteristics of the monotherapy and combination therapy patients. Most of the patients in our study were white men, at approximately 70.25%. Regarding ethnicity, sex, and age, we found no difference between the two groups. The proportion of diabetic patients in patients with monotherapy was higher than that in patients with combination therapy (49.5% versus 33.9%, p= 0.012). The proportions of other comorbid diseases between the 2 groups were similar. Therefore, monotherapy and combination therapy patients have similar Charlson comorbidity indices. Our study ensured the accuracy of microorganism culture results in identifying infections rather than colonization through a comprehensive approach. This included considering clinical diagnosis by physicians, reviewing the clinical histories of infected patients, and conducting a meticulous review of medical records in the MIMIC-IV database to confirm the presence of infections. We included adults with infections caused by CRPA, primarily bacteremia, pneumonia, urinary tract infections, and tissue infections. Sputum was the most common specimen source, followed by urine. In this study, 27 (29.0%) patients receiving monotherapy and 70 (37.6%) patients receiving combination therapy also received ventilation support. Fifty patients with CRPA infections developed septic shock. The rate of clinical success for combination therapy was higher than that of monotherapy (73.1% versus 60.4%, p=0.028). We did not find a significant difference in complete clinical success between the 2 groups (36.2% versus 42.0%, p=0.931).
We also compared different characteristics of clinical failure patients with those of clinical success patients (Table 2). Regarding ethnicity, sex, and age, we found no difference between the two groups. The proportion of renal disease patients in the clinical failure group was higher than that in the clinical success group (37.9% versus 26.0%, p= 0.044). Compared to patients in the clinical failure group, patients in the clinical success group were more likely to die within 28 days after CRPA was found (48.3% versus 3.6%, p<0.001).
Kaplan-Meier analysis
In Fig. 2 (Title: Comparison of All-Cause Mortality within 28 Days After CRPA Detection between Monotherapy and Combination Therapy, legend: This figure compares all-cause mortality within 28 days after CRPA detection for Monotherapy and Combination Therapy. X-axis: Time (days) after CRPA detection. Y-axis: Proportion of surviving patients. Blue curve: Monotherapy. Green curve: Combination Therapy. Log-rank test, p-value = 0.34, indicates no significant difference. At 28 days, 79 survived in Monotherapy, and 151 in Combination Therapy.), no significant difference was observed between patients who received monotherapy and those who received combination therapy for all-cause mortality within 28 days after CRPA was found (21.3% vs. 13.8%).

Comparison of All-Cause Mortality within 28 Days After CRPA Detection between Monotherapy and Combination Therapy
Univariate and multivariate logistic regression models
To verify the effect of monotherapy and combination therapy on clinical efficacy through univariate and multivariate logistic regression analyses, the covariates listed in Table 1 were used. Model 1 is the unadjusted model. Model 2 was adjusted for model 1 plus age ≥60 years, sex, and ethnicity. Model 3 was adjusted for model 2 plus comorbidities: myocardial infarction, chronic pulmonary disease, and renal disease; and model 4 was adjusted for model 3 plus ventilation, septic shock, the SOFA score, and the Charlson comorbidity index (Table 3).
After adjusting each model listed above, monotherapy was found to be significantly correlated with clinical success (model 1: odds ratio (OR), 0.581; 95% confidence interval (CI), 0.354-0.953; p=0.032; model 2: OR, 0.574; 95% CI, 0.336-0.981; p = 0.042; model 3: OR, 0.575; 95% CI, 0.334-0.989; p = 0.046; and model 4: OR, 0.559, 95% CI, 0.321-0.976; p = 0.041). However, we found that monotherapy was not related to complete clinical success (model 1: OR, 0.978; 95% CI, 0.587-1.629; p = 0.931; model 2: OR, 0.988; 95% CI, 0.590-1.655; p = 0.964; model 3: OR, 0.942; 95% CI, 0.554-1.559; p = 0.824; and model 4: OR, 0.661, 95% CI, 0.518-1.517; p = 0.887).
Subgroup analyses
To rule out the potentially confounding influences of gender, SOFA, and Charlson comorbidity index, subgroup analyses were performed (Table 4). Monotherapy may be a risk factor for clinical failure in male patients (OR:0.441, 95%CI:0.215-0.904) or patients with a SOFA ≥2 or a Charlson comorbidity index≥6 (OR: 0.469, 95% CI: 0.231-0.953; and OR: 0.467, 95% CI: 0.222-0.980). We did not find an association between monotherapy and complete clinical success or 28-day mortality.
Discussion
The primary objective of this study is to determine the effectiveness of anti-Infective combination therapy compared to monotherapy in achieving clinical success in patients with CRPA infection and risk factors of clinical failure of monotherapy. In this study, we found that combination therapy is recommended for CRPA infection patients, especially those whose SOFA score was ≥2 or whose Charlson comorbidity index was ≥6. Regarding all-cause 28-day mortality, we did not find any differences between the monotherapy and combination therapy groups.
CRPA has emerged and caused many nosocomial outbreaks, leading to millions of deaths each year [13, 14]. As the carbapenem-resistance mechanisms are complicated, selecting an effective and safe antibiotic regimen remains a challenge. Traditional antipseudomonal β-lactams, including cefepime, ceftazidime and piperacillin/tazobactam and new BLBLIs (ceftazidime-avibactam and ceftolozane-tazobactam), have been found to be effective for CRPA [2, 3]. To increase the success rates of treatment, researchers have attempted to identify the most effective antibiotic regimens against CRPA. In this study, we also found that combination therapy was more effective than monotherapy in patients with CRPA infection. However, the effectiveness of combination therapy for CRPA infections remains controversial. One way of assessing the effectiveness of antibiotic regimens involves in vitro methods based on bacterial killing and antibiotic synergism [15, 16]. According to Ramos JF [4] et al., meropenem with colistin demonstrated superior performance compared to other antibiotic regimens. In vivo CRPA models were also created to test the efficacy of antibiotic regimens. In an intraperitoneal murine CRPA infection model, combination therapy involving colistin and rifampicin exerted a synergistic effect [17]. A previous study demonstrated that the combination of caspofungin and polymyxin exhibited superior efficacy compared to caspofungin alone in reducing mixed biofilm biomass and fungal and bacterial viability in CRPA strains [18]. Similarly, the combination of ceftazidime/avibactam (CZA) with aztreonam (ATM) showed synergistic bacteriostatic or bactericidal activity against NDM-, IMP-, KPC+IMP-, and KPC+NDM-producing carbapenem-resistant Enterobacterales (CRE) strains. This combination therapy not only reduced mortality but also prolonged the lifespan of mice infected with these strains [19]. Furthermore, a combination therapy involving aggressive doses of polymyxin B and tigecycline displayed synergistic or additive effects in treating multidrug-resistant carbapenem-resistant Acinetobacter baumannii(CRAB) infections in humans [20]. In a previous retrospective cohort study included critically ill patients with CRAB infections, they found that patients who received the combination therapy of colistin plus meropenem had a significantly lower adjusted odds ratio (aOR) for 30-day mortality compared to those who received colistin monotherapy. The aOR for 30-day mortality was 0.43, with a 95% confidence interval (CI) ranging from 0.23 to 0.82 [21]. The results of previous study showed that CRAB infections patients who received loading dose (LD) colistin-imipenem had a lower 30-day survival rate (adjusted HR = 0.57, 95% CI: 0.37-0.90; p = 0.015) and a lower clinical response (aHR = 0.56, 95% CI: 0.35-0.90; p = 0.017) compared with those who received LD colistin-meropenem [22].
However, combination therapy did not improve clinical outcomes in all patients with carbapenem-resistant bacteria infection. In a study by Mical Paul [12] et al., which included 406 patients, no significant difference was observed in clinical failure at 14 days after randomization between the colistin monotherapy group (156/198, 79%) and the combination therapy group (152/208, 73%) (risk ratio [RR] 0.93, 95% CI 0.83-1.03). Regarding infections caused by CRAB, the combination of colistin with vancomycin did not show any significant differences in 30-day mortality, clinical response, or microbiological response compared to colistin alone. The rates of nephrotoxicity were similar in both groups, suggesting that colistin combination therapy with vancomycin may not be necessary for managing CRAB infections [23]. A recent meta-analysis that involved 11 studies and 396 patients with carbapenem-resistant gram-negative bacteria (CRGNB) receiving ceftazidime/avibactam alone or in combination was conducted. There was no significant difference in the mortality rate and microbiological cure rate between combination therapy and monotherapy (38.1% vs. 30.9%; 64.9% vs. 63.4%), according to the meta-analysis [24]. In Western China, a retrospective study of 355 patients with Carbapenem-resistant Gram-negative bacterial bloodstream infections (CRGNB-BSI) found that Combination antimicrobial therapy was not superior to monotherapy (P = 0.387) and appropriate therapy was associated with lower treatment failure and 28-day in-hospital mortality rates [25]. Another retrospective study of 164 CRE bloodstream infection cases in China, highlighted the importance of early detection of carbapenemase type and timely initiation of appropriate combination therapy for improving survival [26]. A randomized clinical trial investigated the association between mortality in Acinetobacter baumannii infections and colistin resistance, showed that colistin monotherapy yielded better outcomes compared to colistin-meropenem combination therapy for patients with colistin-resistant isolates [27]. Current guidelines do not take a definitive stance on whether to recommend or discourage the use of combination therapy with new antibiotics (ceftazidime-avibactam and ceftolozane-tazobactam) or cefiderocol for CRPA infections [2, 3]. Overall, these studies underscore the importance of exploring combination therapies to combat carbapenem-resistant bacterial infections. While some combinations show promising results and improved outcomes, it's essential to recognize that not all combination therapies may be effective in every case. The severity of the infection, the specific bacterial strain, and individual patient factors may influence the success of combination therapies. Further research and clinical trials are necessary to identify the most effective treatment strategies for combating carbapenem-resistant bacteria infections.
In addition to finding the most effective antibiotic regimens, identifying the patients who benefit most from monotherapy is also important. Antibiotics can harm patients by various mechanisms: drug toxicity, mitochondrial dysfunction and organ dysfunction, adverse drug reactions, and antimicrobial resistance [8]. Therefore, in order to prevent harm caused by antimicrobials, doctors should limit their use to only when necessary. For patients with non-severe CRPA infections, current guidelines also recommend individualized selection of in vitro-active monotherapy based on the source and type of infection. However, current guidelines do not provide specific tools to evaluate the severity of CRPA infections [2, 3]. SOFA is one of the most frequently used tools to screen and evaluate the severity of sepsis and is also shown to be closely related to the outcomes of sepsis patients [28]. The SOFA score is required for accurate assessment [29]. Combination therapy consisting of two antimicrobials with gram-negative coverage for empiric treatment is recommended for patients with sepsis or septic shock and a high risk for multidrug-resistant (MDR) organisms [30]. In our study, we also found that combination therapy is beneficial for CRPA-infected patients whose SOFA score was ≥ 2 points to control infection. Similarly, SOFA is recommended to help physicians evaluate clinical CRE infection severity before meropenem-based combination therapy is performed [31].
In addition to organ dysfunction, disease burden should be taken into consideration when physicians evaluate the outcomes of infection. The Charlson comorbidity index has been a useful, simple, and readily applicable tool for physicians in their effort to assess and underline complicated diseases and an indicator of disease burden. Its weighted score was assigned to 17 comorbidities and ages, which were found to be associated with long-term mortality [32]. Patients with weakened immune systems or existing health conditions are more vulnerable to P. aeruginosa and are at greater risk of developing severe infections like septic shock or sepsis [33,34,35]. The presence of comorbidities is a crucial factor that affects the prognosis of respiratory system infections. Comorbidities such as cardiovascular disease and cancer, which are included in the Charlson comorbidity index, were associated with worse outcomes in cases of acute respiratory infections [36, 37]. The administration of appropriate antimicrobials is one of the most important interventions to control the infection.
In this study, we also explored which antimicrobial regimen (monotherapy or combination therapy) was beneficial to achieving clinical anti-infection treatment success for those patients who had more comorbid diseases. According to the subgroup analysis results, we further found that combination therapy is more suitable for CRPA-infected patients whose Charlson comorbidity index is not less than 6 to control infection.
Our study has the following limitations. First, it is a retrospective study from a large database, and further random control trials are needed. Second, the data was obtained from the MIMIC-IV database,which may limit the generalizability of the findings to other settings. Different hospitals or regions may have variations in patient populations, treatment protocols, and antimicrobial resistance patterns, which could affect the outcomes. Third, the study included a relatively small sample size (279 subjects), which may limit the statistical power and generalizability of the findings. A larger sample size would provide more robust results and allow for more detailed subgroup analyses. Forth, there are some P. aeruginosa antibiotic susceptibilities results that do not include β-lactam agent, so we do not know if β-lactams are effective against these P. aeruginosa bacteria in vitro.Fifth, potential unmeasured confounders: Despite adjusting for various factors in the multivariate analysis, there may still be unmeasured confounding variables that were not accounted for. These variables could potentially influence the outcomes and introduce bias into the results. Sixth,we had no access to the specific carbapenem-resistance mechanisms of CRPA isolated from patients in our study. Seventh, we did not find the most effective combination therapy regimens for CRPA due to the limitation in the original data.
Conclusion
Combination therapy is more effective for CRPA infection patients, especially those whose SOFA score is ≥ 2 or whose Charlson comorbidity index is ≥ 6. SOFA and Charlson comorbidity index may help clinicians to decide antibiotic regimen and to avoid using unnecessary antibiotics.
Availability of data and materials
Anyone should be obliged to complete the training course to gain access to the database. Data associated with this study has been deposited. The data are available on the MIMIC-IV database website at https://mimic-iv.mit.edu/.
References
Brink AJ. Epidemiology of carbapenem-resistant Gram-negative infections globally. Curr Opin Infect Dis. 2019;32(6):609–16.
Paul M, Carrara E, Retamar P, Tangden T, Bitterman R, Bonomo RA, de Waele J, Daikos GL, Akova M, Harbarth S, et al. European society of clinical microbiology and infectious diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant gram-negative bacilli (endorsed by European society of intensive care medicine). Clin Microbiol Infect. 2022;28(4):521–47.
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clin Infect Dis. 2023:ciad428.
Ramos JF, Leite G, Martins RCR, Rizek C, Al Sanabani SS, Rossi F, Guimaraes T, Levin AS, Rocha V. Costa SF Clinical outcome from hematopoietic cell transplant patients with bloodstream infection caused by carbapenem-resistant P aeruginosa and the impact of antimicrobial combination in vitro. Eur J Clin Microbiol Infect Dis. 2022;41(2):313–7.
Khawcharoenporn T, Pruetpongpun N, Tiamsak P, Rutchanawech S, Mundy LM, Apisarnthanarak A. Colistin-based treatment for extensively drug-resistant Acinetobacter baumannii pneumonia. Int J Antimicrob Agents. 2014;43(4):378–82.
Memar MY, Adibkia K, Farajnia S, Samadi Kafil H, Khalili Y, Azargun R, Ghotaslou R. In-vitro effect of imipenem, fosfomycin, colistin, and gentamicin combination against carbapenem-resistant and biofilm-forming pseudomonas aeruginosa isolated from Burn Patients. Iran J Pharm Res. 2021;20(2):286–96.
Rigatto MH, Vieira FJ, Antochevis LC, Behle TF, Lopes NT, Zavascki AP. Polymyxin B in combination with antimicrobials lacking in vitro activity versus polymyxin b in monotherapy in critically ill patients with acinetobacter baumannii or pseudomonas aeruginosa infections. Antimicrob Agents Chemother. 2015;59(10):6575–80.
Arulkumaran N, Routledge M, Schlebusch S, Lipman J, Conway Morris A. Antimicrobial-associated harm in critical care: a narrative review. Intensive Care Med. 2020;46(2):225–35.
Kett DH, Cano E, Quartin AA, Mangino JE, Zervos MJ, Peyrani P, Cely CM, Ford KD, Scerpella EG, Ramirez JA, et al. Implementation of guidelines for management of possible multidrug-resistant pneumonia in intensive care: an observational, multicentre cohort study. Lancet Infect Dis. 2011;11(3):181–9.
Yadav H, Harrison AM, Hanson AC, Gajic O, Kor DJ, Cartin-Ceba R. Improving the accuracy of cardiovascular component of the sequential organ failure assessment score. Crit Care Med. 2015;43(7):1449–57.
Jentzer JC, Wiley B, Bennett C, Murphree DH, Keegan MT, Kashani KB, Bell MR, Barsness GW. Temporal trends and clinical outcomes associated with vasopressor and inotrope use in the cardiac intensive care unit. Shock. 2020;53(4):452–9.
Paul M, Daikos GL, Durante-Mangoni E, Yahav D, Carmeli Y, Benattar YD, Skiada A, Andini R, Eliakim-Raz N, Nutman A, et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: an open-label, randomised controlled trial. Lancet Infect Dis. 2018;18(4):391–400.
Cornaglia G, Mazzariol A, Lauretti L, Rossolini GM, Fontana R. Hospital outbreak of carbapenem-resistant Pseudomonas aeruginosa producing VIM-1, a novel transferable metallo-beta-lactamase. Clin Infect Dis. 2000;31(5):1119–25.
Kang CI, Kim SH, Kim HB, Park SW, Choe YJ, Oh MD, Kim EC, Choe KW. Pseudomonas aeruginosa bacteremia: risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin Infect Dis. 2003;37(6):745–51.
Sopirala MM, Mangino JE, Gebreyes WA, Biller B, Bannerman T, Balada-Llasat JM, Pancholi P. Synergy testing by Etest, microdilution checkerboard, and time-kill methods for pan-drug-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2010;54(11):4678–83.
Scudeller L, Righi E, Chiamenti M, Bragantini D, Menchinelli G, Cattaneo P, Giske CG, Lodise T, Sanguinetti M, Piddock LJV, et al. Systematic review and meta-analysis of in vitro efficacy of antibiotic combination therapy against carbapenem-resistant Gram-negative bacilli. Int J Antimicrob Agents. 2021;57(5):106344.
Cai Y, Yang D, Wang J, Wang R. Activity of colistin alone or in combination with rifampicin or meropenem in a carbapenem-resistant bioluminescent Pseudomonas aeruginosa intraperitoneal murine infection model. J Antimicrob Chemother. 2018;73(2):456–61.
Fortes BN, Scheunemann G, de Azevedo Melo AS, Ishida K. Caspofungin alone or combined with polymyxin B are effective against mixed biofilm of Aspergillus fumigatus and carbapenem-resistant Pseudomonas aeruginosa. Res Microbiol. 2023;174(1–2):103993.
Lu G, Tang H, Xia Z, Yang W, Xu H, Liu Z, Ni S, Wang Z, Shen J. In vitro and in vivo Antimicrobial Activities of Ceftazidime/Avibactam Alone or in Combination with Aztreonam Against Carbapenem-Resistant Enterobacterales. Infect Drug Resist. 2022;15:7107–16.
Hagihara M, Housman ST, Nicolau DP, Kuti JL. In vitro pharmacodynamics of polymyxin B and tigecycline alone and in combination against carbapenem-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2014;58(2):874–9.
Katip W, Uitrakul S, Oberdorfer P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: A Propensity Score-Matched Analysis. Antibiotics Basel. 2020;9(10):647.
Katip W, Oberdorfer P, Kasatpibal N. Effectiveness and Nephrotoxicity of Loading Dose Colistin-Meropenem versus Loading Dose Colistin-Imipenem in the Treatment of Carbapenem-Resistant Acinetobacter baumannii Infection. Pharmaceutics. 2022;14(6):1266.
Katip W, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of Colistin Alone versus Colistin Plus Vancomycin in Critically Ill Patients Infected with Carbapenem-Resistant Acinetobacter baumannii: A Propensity Score-Matched Analysis. Pharmaceutics. 2021;13(2):162.
Onorato L, Di Caprio G, Signoriello S, Coppola N. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant Gram-negative bacteria: A meta-analysis. Int J Antimicrob Agents. 2019;54(6):735–40.
Qu J, Feng C, Li H, Lv X. Antibiotic strategies and clinical outcomes for patients with carbapenem-resistant Gram-negative bacterial bloodstream infection. Int J Antimicrob Agents. 2021;57(3): 106284.
Wang X, Wang Q, Cao B, Sun S, Zhang Y, Gu B, Li B, Liao K, Zhao F, Jin L, et al. Retrospective Observational Study from a Chinese Network of the Impact of Combination Therapy versus Monotherapy on Mortality from Carbapenem-Resistant Enterobacteriaceae Bacteremia. Antimicrob Agents Chemother. 2018;63(1):e01511–18.
Dickstein Y, Lellouche J, Amar MBD, Schwartz D, Nutman A, Daitch V, Yahav D, Leibovici L, Skiada A, Antoniadou A, et al. Treatment outcomes of colistin and carbapenem resistant acinetobacter baumannii infections an exploratory subgroup analysis of a randomized clinical Trial. Clin Infect Dis. 2019;69(5):769–76.
Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23(1):374.
Vincent JL, de Mendonca A, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F, Blecher S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units results of a multicenter, prospective study Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26(11):1793–800.
Rehn M, Chew MS, Olkkola KT, Ingi Sigurethsson M, Yli-Hankala A, Hylander Moller M. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock in adults 2021 - endorsement by the Scandinavian society of anaesthesiology and intensive care medicine. Acta Anaesthesiol Scand. 2022;66(5):634–5.
Pascale R, Giannella M, Bartoletti M, Viale P, Pea F. Use of meropenem in treating carbapenem-resistant Enterobacteriaceae infections. Expert Rev Anti Infect Ther. 2019;17(10):819–27.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Kang CI, Kim SH, Park WB, Lee KD, Kim HB, Kim EC, Oh MD, Choe KW. Bloodstream infections caused by antibiotic-resistant gram-negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–6.
Lin KY, Lauderdale TL, Wang JT, Chang SC. Carbapenem-resistant Pseudomonas aeruginosa in Taiwan: Prevalence, risk factors, and impact on outcome of infections. J Microbiol Immunol Infect. 2016;49(1):52–9.
Tam VH, Gamez EA, Weston JS, Gerard LN, Larocco MT, Caeiro JP, Gentry LO, Garey KW. Outcomes of bacteremia due to Pseudomonas aeruginosa with reduced susceptibility to piperacillin-tazobactam: implications on the appropriateness of the resistance breakpoint. Clin Infect Dis. 2008;46(6):862–7.
Setter NW, Peres ML, de Almeida BMM, Petterle RR, Raboni SM. Charlson comorbidity index scores and in-hospital prognosis of patients with severe acute respiratory infections. Intern Med J. 2020;50(6):691–7.
Varol Y, Hakoglu B, Kadri Cirak A, Polat G, Komurcuoglu B, Akkol B, Atasoy C, Bayramic E, Balci G, Ataman S, et al. The impact of charlson comorbidity index on mortality from SARS-CoV-2 virus infection and A novel COVID-19 mortality index: CoLACD. Int J Clin Pract. 2021;75(4):e13858.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
L, C, J L acquired the data,drafted and revised the manuscript. JZ W and Y J and YM L designed the study, provided supervision and critically revised the manuscript. All authors approve the final version of the manuscript and agree to be accountable for all aspects of the study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project was approved by the Institutional Review Boards of Beth Israel Deaconess Medical Center (Boston, MA, USA) and the Massachusetts Institute of Technology (Cambridge, MA, USA). The collection of patient information and creation of the research resource was reviewed by the Institutional Review Board at the Beth Israel Deaconess Medical Center, who granted a waiver of informed consent and approved the data sharing initiative. The study authors had complete the CITI Program course (Human Research and Data or Specimens Only Research) to gain access to the database (Record ID: 47755805). The information of patients in this study is deidentified and anonymous. Individual permission was not required for this retrospective analysis. All methods were performed in accordance with the relevant guidelines and regulations. We have currently gone through the course to obtain permission from the ethics committee mentioned above to obtain information of deidentified patients from the database, not from the authors' hospital, so this study may only require approval from the committee above, not the the ethics committee affiliated to authors.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, J., Lin, J., Weng, J. et al. Clinical success of anti-infective combination therapy compare to monotherapy in patients with carbapenem-resistant Pseudomonas aeruginosa infection: a 10-years retrospective study. BMC Infect Dis 24, 248 (2024). https://doi.org/10.1186/s12879-024-09060-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09060-2