
Abstract
Background objective
This study aimed to understand the basic situation of adults with human immunodeficiency virus (HIV) receiving antiretroviral therapy (ART) in Meigu County, Liangshan Yi Autonomous Prefecture. The information of patients who had been on ART for more than 6 months, the effect of ART, the possible reasons for ART failure, knowledge of drug resistance among patients with ART failure and the possible reasons for the emergence of drug resistance were analyzed.
Methods
A total of 2753 people living with HIV (PLWH) were collected for HIV-1 RNA virus nucleic acid testing. Plasma specimens with HIV-1 RNA ≥ 1000 copies/mL were sent to the laboratory for nucleic acid extraction, PCR, electrophoresis and sequencing, and the sequencing results were submitted to the HIV drug resistance database of Stanford University for subtyping to determine the drug resistance mutation sites and drug sensitivity levels.
Results
A total of 2753 patients were enrolled in this study. Antiviral therapy failed in 288 patients and was successfully amplified in 245, of which 111 had resistance genes. The resistance rate to failure of viral suppression was 45.3% (111/245). The highest rates of resistance to NNRTIs were found for efavirenz (EFV) and nevirapine (NVP) (42.9%), and the highest rates of resistance to NRTIs were found for 3TC and emtricitabine (FTC) (15.9%). The most common NNRTI resistance mutation site was K103N (20.8%), followed by V179D (9.4%) and V106M (7.8%); the most common NRTI resistance mutation site was M184V/I/MV (14.3%), followed by K65R (6.9%); three PI-associated resistance mutation sites were identified. The subtype of the resistant strain was CRF07-BC in almost all patients (98.9%).
Conclusions
Compared with the previous low ART efficacy in the county, this study showed that the overall virological failure (VF) resistance rate in the county is still low, dominated by resistance to EFV, NVP, 3TC, FTC, and didanosine (DDI). Due to economic constraints, the core regimen is still 3TC + TDF, but before initiating ART, testing for HIV-1 subtypes and resistance should be conducted to avoid resistance that can lead to VF, especially for patients with high risk factors for resistance as shown by epidemiologic investigations.
Similar content being viewed by others


Background
Acquired immunodeficiency syndrome (AIDS) is a chronic infectious disease caused by human immunodeficiency virus (HIV). At present, antiretroviral therapy (ART) in China has made great progress, but in some remote mountainous areas, free drugs provided by the state are still used as the main medications, and with the prolongation of medication use, these drugs have an increased risk of drug resistance, which reduces the therapeutic effect and makes it difficult to achieve the goal of 95% HIV/AIDS control. Therefore, this study focused on Meigu County in Liangshan Prefecture, Sichuan Province, China, which is dominated by the Yi ethnic group, is a high-incidence area of the AIDS epidemic, and has a low economic development level. This study analyzed HIV-1 RNA, HIV-1 RNA resistance genes, and resistance-related risk factors in patients aged 18 years and older who had been on regular ART for more than 6 months, with the aim of providing a reference for the future development of ART regimens in this area.
Methods
Study participants
Medical staff called all candidate participants in the district using ART to introduce them to this study and to confirm their eligibility for participation. All participants signed an informed consent form prior to enrollment. Finally, a total of 2753 people living with HIV (PLWH) were enrolled in this study. A total of 2753 plasma samples were collected from HIV/AIDS patients aged 18 years and older in the district who had received ART for ≥6 months from January 1, 2010, to January 1, 2021, and the plasma was derived from specimens tested annually at regular intervals.
Source
Data were obtained from the Chinese Center for Disease Control and Prevention Integrated AIDS Prevention and Control Information System, including patient name, sex, age, education level, marital status, family type, HIV transmission route, first CD4+ counts, treatment duration, and treatment regimen.
Collection, preservation and transportation of plasma
Two milliliters of peripheral venous blood from the subject was drawn using a sterile syringe and injected into a sterile collection tube containing ethylenediaminetetraacetic acid (EDTA), and the patient’s plasma was separated by centrifugation at 1600 rpm for 5–20 minutes. Fresh plasma was drawn and injected into another sterile centrifuge tube for backup, and the sample could be used immediately for testing. The samples could be stored at − 70 °C for a long time for backup, avoiding repeated freezing and thawing, and were transported in a jug with ice or a foam box with ice after sealing.
Experimental steps
Viral load detection
Viral load (VL) was detected in the plasma of the study subjects using a fully automated nucleic acid extractor AU1001–96 (Wuxi Biotec Biotechnology Co., Ltd.), and the performance of the assay was strictly in accordance with the instruction manual of the assay system. Virological failure (VF) was defined as a viral load ≥1000 copies/ml in an individual on ART for more than 6 months [1]. Plasma samples from VF patients were selected for the next step of genotypic drug resistance monitoring.
Genetic resistance testing
HIV genotypic resistance testing was performed on plasma with a viral load ≥1000 cp/ml using a laboratory self-constructed assay (in-house).
-
① Nucleic acid extraction: RNA was extracted using a MagNA Pure LC 2.0 fully automated nucleic acid extractor and MagNA Pure LC Total Nucleic Acid Isolation Kit, which is a high-performance reagent kit [Roche (Switzerland)].
-
② PCR: Using the extracted RNA as a template, the HIV-1 pol gene region was amplified by nested PCR with a length of 1200 bp, including the protease and reverse transcriptase regions, and the first round of PCR was performed using the AccessQuick RT–PCR System (A1702) kit (ProMag (Beijing) Biotechnology Co. Ltd.]); the above two PCR products were amplified using an Eppendorf 5333–47,507 PCR instrument (Eppendorf (Germany)).
-
③ Electrophoresis and sequencing: The PCR products were amplified by 1% agarose gel electrophoresis using a capillary electrophoresis instrument (QIAxcel Advanced, Germany) to confirm the correct molecular weight of the amplified fragments, and then the amplified products were sent to Beijing Noce Genome Research Center Co. The amplification and sequencing primers are shown in Table 1.
Definition of indicators
Referring to the 2013 WHO “Comprehensive guidelines for the use of antiretroviral drugs in the treatment and prevention of HIV infection”, the drug resistance rate = the number of resistant drugs/(number of investigations - number of amplification negatives)*100%, and the rate of resistance to viral suppression failure = the number of resistant drugs/(number of viral suppression failures - number of amplification negatives)*100%.
Sequence analysis
The measured sequences were edited and spliced by ChromasPro 1.33 software and corrected by BioEdit software(Ibis Biosciences, Carlsbad, CA, USA), and the spliced sequences were submitted to the Stanford HIV drug resistance database (http://hivdb.stanford.edu) for subtyping to determine the drug resistance mutation sites and drug sensitivity levels. The Stanford University (HIVDB) system is categorized into five degrees of drug resistance according to the degree of drug resistance: sensitive (S), potentially resistant (P), low resistant (L), moderately resistant (I), and highly resistant (H) (https://hivdb.stanford.edu/).
Statistical processing
The sociodemographic information of all study subjects was summarized, organized and analyzed using an Excel sheet, and SPSS 25.0 was used for descriptive and statistical analyses. Indicators such as the rate, composition ratio, mean and standard deviation were used to describe the basic information of AIDS patients. The variables were first subjected to a one-way chi-squared (χ2) test, and the group of variables with P < 0.05 was included in the multivariate logistic regression. The samples with virological failure and successful amplification were divided into drug-resistant and nondrug-resistant groups, and the variables were first compared between the two groups by the one-way chi-squared (χ2) test or Fisher’s exact test for statistical significance. The variables with P < 0.05 were again analyzed by multivariate logistic regression for the influence of the occurrence of drug resistance in patients, with a difference with P < 0.05 considered statistically significant.
Results
Sociodemographic information
As of January 1, 2021, there were 2753 HIV/AIDS patients aged 18 years and older who had been on ART for more than 6 months in Meigu County. Among them, 1697 (61.6%) were male; 2609 (94.8%) were aged 18–49 years; 2064 patients had not attended school (75.0%); 1834 had a spouse (66.6%); sexual transmission and intravenous drug transmission accounted for half each; first CD4+ counts of under 200 counts/μl occurred in 381 cases (13.8%), 200–349 counts/μl in 1787 cases (28.6%), 350–499 counts/μl in 1721 cases (26.2%), and 500 counts/μl and above in 864 cases (31.4%); an initial ART regimen with tenofovir disoproxil fumarate+lamivudine (TDF + 3TC) as the core drug was used in 2541 patients (93.3%) and non-TDF + 3TC as the core drug in 212 patients (7.7%); and the time on ART was 6 months-2 years for 1720 patients (62.5%), and the remaining patients were treated for more than 2 years (37.5%, 1033/2753). Specific information is shown in Table 2.
Initial ART regimen
The primary ART regimen in the district is the standard first-line regimen of the National Antiviral Program (TDF or AZT + 3TC + EFV/NVP), with rare use of TDF or AZT + 3TC + LPV/r regimens or other antiviral drugs.
Analysis of the causes of virological failure
One-way chi-square (χ2) tests or Fisher’s exact tests were used to analyze the effect of patient sex, mode of transmission, first CD4+ counts, initial ART regimen, and time on ART, which were significantly associated with the risk of VF, on ART (P < 0.05), as shown in Table 3.
Further multivariate logistic regression analysis of statistically significant ART outcome variables showed that the risk of VF was 1.96 times higher among men than among women (odds ratio (OR): 1.96, 95% confidence interval (CI): 1.38–2.79); first, CD4+ counts were a protective factor for ART, and the higher the CD4+ counts were, the lower the rate of VF, as shown in Table 4.
Drug resistance situation
Sociodemographic information of drug-resistant patients
Among 2753 AIDS patients who had received ART for more than 6 months, 288 patients were found to have VF, 245 samples were successfully amplified, and the amplification success rate was 85.1% (245/288), of which 111 samples had different degrees of resistance to a certain antiviral drug, and the overall resistance rate in this area was 4.1% (111/2710). Among the 111 resistant patients, more than half were male, the 18–49 age group was predominant, most patients were illiterate, sexual transmission and injection drug transmission accounted for almost half of transmission, and the highest rate of resistance was found among patients with first CD4+ counts under 200 counts/μl, with more than 90% of patients on TDF + 3TC as the initial core drug regimen. A total of 68.5% of patients had a change in ART regimen while on medication. The details are shown in Table 5.
Types of drug resistance
Among 111 resistant patients, only 3 were found to be resistant to some NRTIs, 66 were found to be resistant to some non-nucleoside reverse transcriptase inhibitors (NNRTIs), and 2 were found to be resistant to some protease inhibitors (PIs); 37 were found to be resistant to both nucleoside reverse transcriptase inhibitors (NRTIs) and NNRTIs, 1 was found to be resistant to both NNRTIs and PIs, and no one was resistant to both NRTIs and PIs; only 1 was found to be resistant to NRTIs, NNRTIs and PIs simultaneously. The information is shown in Fig. 1.

Different types of drug resistance
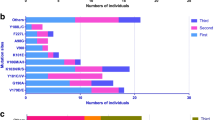
Degree of resistance to different drugs
Among the NRTIs, resistance to 7 different drugs was found, namely, abacavir (ABC), zidovudine (AZT), stavudine (D4T), desoxymesterol (DDI), emtricitabine (FTC), lamivudine (3TC), and tenofovir (TDF), and 39 participants were resistant to both FTC and 3TC, of which 35 were highly resistant and 4 were moderately resistant. Among the NNRTIs, resistance to 5 different drugs was found, namely, doravirine (DOR), efavirenz (EFV), nevirapine (NVP), etravirine (ETR), and rilpivirine (RPV). A total of 105 participants were resistant to both EFV and NVP, of which 87 were highly resistant, 1 was moderately resistant, and 17 were potentially resistant. Among the PIs, resistance to 7 different drugs was found, namely, atazanavir/ritonavir (ATV/r), fosamprenavir/ritonavir (FPV/r), indinavir/ritonavir (IDV/r), lopinavir/ritonavir (LPV/r), nelfinavir (NFV), saquinavir/ritonavir (SQV/r), and tipranavir/ritonavir (TPV/r). Four participants were resistant to both NFV and TPV/r, of which four were potentially resistant to NFV, three had low resistance to TPV/r, and one was potentially resistant to ATV/r. The degree of resistance to different drugs is shown in Fig. 2.

Different drug resistance levels
Subtype distribution
Among 245 samples, 243 were of the CRF07-BC subtype, accounting for 99.1%, 1 sample was of the CRF01_AE subtype, and 1 sample was of the CRF83-cpx subtype.
Drug resistance mutations
Among the 245 successfully amplified samples, 23 NRTI-associated drug resistance mutations were identified, of which the most common was the M184V mutation, accounting for 12.2% (30/245), followed by the K65R mutation, accounting for 6.9% (17/245); 28 NNRTI-associated drug resistance mutations were identified, of which the most common was K103N, accounting for 20.8%, followed by the V179D and V106M mutations, accounting for 9.4 and 7.8%, respectively; and 3 PI-associated drug resistance mutation sites were identified, accounting for 9.4 and 7.8%. The most common mutation was K103N, accounting for 20.8%, followed by V179D and V106M, accounting for 9.4 and 7.8%, respectively; three PI-related resistance mutations were identified: one major mutation was M46MIL, and two minor mutations were Q58E and L33LF. The details are shown in Figs. 3 and 4.

NRTI-related mutation site information

NNRTI-related mutation site information
Analysis of the causes of drug resistance
To analyze the possible causes of drug resistance, 245 successfully amplified samples were divided into nonresistant and resistant groups according to whether they were resistant, and analysis by one-way chi-square (χ2) test or Fisher’s exact test revealed that patient sex, age group, education level, mode of transmission, family type, initial ART regimen, and time on ART were not related to the occurrence of drug resistance, while patient marital status, first CD4+ counts and whether the ART regimen had been changed had a statistically significant effect on drug resistance. The details are shown in Table 6.
Further multifactorial logistic analysis of statistically significant variables for drug resistance revealed that the first CD4+ counts were a protective factor against drug resistance, with higher CD4+ counts associated with a lower incidence of drug resistance; changing the ART regimen was a risk factor for drug resistance, with the risk of resistance with a change in ART while on medication being 2.10 times higher than without a change (OR: 2.10, 95% CI: 1.12–3.91). The details are shown in Table 7.
Discussion
With the comprehensive development of AIDS prevention and control in remote areas of China and the popularization of HIV ART, HIV drug resistance was bound to emerge, and this will affect the efficacy of HIV treatment; therefore, it is very important to analyze the prevalence of drug resistance to guide the formulation of ART regimens in a timely manner. In this study, the ART efficacy and drug resistance of HIV patients in Meigu County who had been regularly using ART for more than 6 months were analyzed.
In this district, patient sex, mode of transmission, first CD4+ counts, initial ART regimen, and time on ART affected the outcome of ART, and further multivariate logistic regression of these factors showed that male sex was a risk factor for VF. The first CD4+ counts were protective, and the higher the CD4+ counts were, the lower the VF rate. Possible reasons why men are more likely to fail ART include the following: women have better healthcare behaviors [2]; women have a lower body mass index than men and can maintain higher drug concentration levels in the body and are more likely to achieve virologic suppression [3]; and the presence of adverse behaviors such as smoking in men can affect viral load control [4]. High CD4+ counts and high viral load suppression make ART more likely to be successful [5], and the initiation of antiviral therapy in patients with CD4+ counts above 500 cells/μl significantly reduces the combined endpoint events of mortality and morbidity [5, 6] and reduces the risk of drug resistance [7], reduced CD4+ counts, impaired cellular immune function, and immunity. The more severe the deficiency, the longer the required immune reconstitution takes and the higher the failure rate of ART, based on which it is recommended that ART be initiated rapidly in patients with HIV/AIDS [8, 9].
In this district, 288 cases of ART failure were found, 245 samples were successfully amplified, 111 samples were resistant to a drug, and the viral suppression failure resistance rate was 45.3%, which was higher than the statewide viral suppression failure resistance rates from 2016 to 2019 (25.3, 22.5, 37.7, 35.0%) [10] and lower than the Dazhou 2019 and Guangyuan 2012–2016 virological failure resistance rates [11, 12]. Of the 245 samples successfully amplified in this region, 42.9% of patients were resistant to NNRTIs (105/111), 16.3% were resistant to NRTIs (40/111), and 4.5% were resistant to PIs (5/111). A total of 105 patients showed resistance to both EFV and NVP, of which 87 were highly resistant, and 39 showed resistance to both 3TC and FTC, among whom 35 were highly resistant. In terms of resistance mutations, the most common resistance mutation for NNRTIs was K103N (20.8%, 51/245). In this region, patient marital status, first CD4+ counts, and whether the medication was changed during treatment had a statistically significant effect on drug resistance. Further multivariate logistic regression analysis of these factors was conducted, and patients’ first CD4+ counts and whether medication was changed during treatment still had an effect on drug resistance. The first CD4+ counts was a protective factor against drug resistance; the higher the CD4+ counts were, the lower the incidence of drug resistance. Changing the ART regimen was a risk factor for drug resistance. Patients may change regimens due to virological failure, adverse drug reactions, and toxic side effects, and these patients may have risk factors such as poor adherence and missed doses that lead to drug resistance [13].
As of January 1, 2021, the viral suppression rate of adult HIV/AIDS patients in Meigu County who had been on antiviral therapy for more than 6 months was 89.5% (2465/2753), with a low overall resistance rate but a high rate of viral suppression failure [3]. The demographic characteristics of the patients in this study showed that more than half of the patients were male (61.6%, 1697/2753), and the majority of them were aged 18–49 years (94.8%, 2609/2753). It is necessary to focus on young adult male patients in the district because the economic development of the district is poor, and it is common for adult male patients to go out to work, oftentimes in unfixed locations and places, so it is difficult to ensure that these people take oral antiviral drugs on time and in the right amount. This group of patients may have missed doses, poor compliance and other factors that increase the risk of drug resistance. This portion of the population may have a unique sexual situation, and long-term working couples are often separated from each other. There may be high-risk nonmarital sex resulting in the spread of the virus, for which mobile population antiviral management follow-up should be improved. Most of the patients in this district did not attend school, and some studies have shown that those with low literacy and low knowledge of AIDS [14] and poor awareness of prevention will be more likely to be infected with HIV. Thus, it is necessary to strengthen the popularization of AIDS-related knowledge in the population and strengthen compliance among HIV/AIDS patients. Among patients who failed ART and developed drug resistance, EFV, NVP, 3TC, FTC, and DDI resistance were predominant, arising from the fact that most patients’ ART regimen was the nationally recommended first-line ART regimen comprising TDF or AZT + 3TC + EFV/NVP, suggesting that patients who failed ART and developed drug resistance in this district could change to the second-line ART regimen of TDF or AZT + 3TC + LPV/r. There were 4 cases of PI drug resistance in the district and 3 cases of Q58 drug resistance mutation, suggesting that TDR may be in use in the district, and the use of such second-line drugs in the population will increase the difficulty of AIDS prevention and treatment. The district needs to increase drug resistance monitoring and strengthen AIDS prevention and treatment management to prevent the spread of PI drug-resistant strains in the population.
The data on HIV/AIDS patients in this study were obtained from the Chinese Center for Disease Control and Prevention Integrated AIDS Prevention and Control Information System, and no specific demographic survey was conducted, which may have led to information bias affecting the analysis results. In this study, only patients with a viral load ≥1000 copies/ml were tested for drug resistance, but patients with a viral load between 51 and 999 copies/ml may also have drug resistance [15], and more sensitive methods can be explored in future studies to improve the detection rate of drug resistance and achieve the goal of ending the AIDS epidemic by 2030 at an early stage [16].
Conclusions
The prevention and treatment of AIDS in the district has seen gradual progress, and the overall drug resistance rate is low, but the VF drug resistance rate is higher than the statewide VF drug resistance rate. VF and the occurrence of drug resistance in patients to EFV, NVP, 3TC, FTC, and DDI is dominant because most of the patients have used the first-line antiretroviral regimen TDF or AZT + 3TC + EFV/NVP and 3TC + EFV/NVP, suggesting that patients with VF and drug resistance in this region can instead use second-line antiviral regimens comprising TDF or AZT + 3TC + LPV/r. Integrase strand transfer inhibitors (INSTIs) have become the first choice among antiviral regimens recommended in the international guidelines for the treatment of AIDS [5], and due to the relatively poor economic development of the region, INSTIs have been included in the national health insurance, but few patients and families can afford the expense. If INSTIs are included in the national free antiretroviral program, further progress in AIDS prevention and treatment in this district may be achieved. At the same time, before ART, HIV-1 subtype and drug resistance testing should be carried out to guide the choice of ART to reduce VF and drug resistance, and the effectiveness of ART in the district will be further improved. This study showed that the viral suppression rate in this district is still far from 95%, although the overall viral resistance rate is not high; the viral suppression failure resistance rate is high, mainly due to the drugs in the first-line free program, so increasing the knowledge of AIDS for patients in this district, improving the level of medical care, and strengthening the management of ART and population mobility are still top priorities.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HIV:
-
Human immunodeficiency virus
- AIDS:
-
Acquired immune deficiency syndrome
- ART:
-
Antiretroviral therapy
- WHO:
-
World health organization
- PLWH:
-
People living with HIV
- EDTA:
-
Ethylenediaminetetraacetic acid
- VL:
-
Viral load
- VF:
-
Virological failure
- HIVDB:
-
HIV drug resistance database
- RT-PCR:
-
Reverse transcription-polymerase chain reaction
- CI:
-
Confidence interval
- OR:
-
Odds ratios
- NNRTI:
-
Nonnucleoside reverse transcriptase inhibitor
- NRTI:
-
Nucleoside reverse transcriptase inhibitor
- PI:
-
Protease inhibitor
- INSTI:
-
Integrase strand transfer inhibitor
- TDF:
-
Tenofovir
- 3TC:
-
Lamivudine
- NVP:
-
Nevirapine
- DOR:
-
Doravinine
- ETR:
-
Etravirine
- EFV:
-
Efavirenz
- AZT:
-
Zidovudine
- LPV/r:
-
Tipranavir/ritonavir
- ATV/r:
-
Atazanavir/ritonavir
- DRv/r:
-
Darunavir/ritonavir
- FPV/r:
-
Tipranavir/ritonavir
- IDV/r:
-
Indinavir/Ritonavir
- NFV:
-
Nelfinavir
- SQV/r:
-
Ritonavir-boosted saquinavir
- TPV/r:
-
Tipranavir/ritonavir
- ABC:
-
Abacavir
- D4T:
-
Stavudine
- DDI:
-
Didanosine
- FTC:
-
Emtricitabine
- ETR:
-
Etravirine
References
Ndahimana J, Riedel DJ, Mwumvaneza M, Sebuhoro D, Uwimbabazi JC, Kubwimana M, et al. Drug resistance mutations after the first 12 months on antiretroviral therapy and determinants of virological failure in Rwanda. Tropical Med Int Health. 2016;21:928–35.
Tran DA, Wilson DP, Shakeshaft A, Ngo AD, Doran C, Zhang L. Determinants of virological failure after 1 year’s antiretroviral therapy in vietnamese people with HIV: findings from a retrospective cohort of 13 outpatient clinics in six provinces. Sex Transm Infect. 2014;90:538–44.
Yuan D, Liu M, Jia P, Li Y, Huang Y, Ye L, et al. Prevalence and determinants of virological failure, genetic diversity and drug resistance among people living with HIV in a minority area in China: a population-based study. BMC Infect Dis. 2020;20:443.
Jordan MR, La H, Nguyen HD, Sheehan H, Lien TT, Duong DV, et al. Correlates of HIV-1 viral suppression in a cohort of HIV-positive drug users receiving antiretroviral therapy in Hanoi, Vietnam. Int J STD AIDS. 2009;20:418–22.
Byonanebye DM, Semitala FC, Katende J, Bakenga A, Arinaitwe I, Kyambadde P, et al. High viral suppression and low attrition in healthy HIV-infected patients initiated on ART with CD4 above 500 cells/μL in a program setting in Uganda. Afr Health Sci. 2020;20:132–41.
Dorward J, Sookrajh Y, Gate K, Khubone T, Mtshaka N, Mlisana K, et al. HIV treatment outcomes among people with initiation CD4 counts >500 cells/μL after implementation of treat all in south African public clinics: a retrospective cohort study. J Int AIDS Soc. 2020;23:e25479.
Li H, Du B, Tian X, Liu W, Yao W. DNA drug resistance and subtypes in HIV-1 patients receiving antiretroviral therapy in Fuxin, Liaoning China. Trop Med. 2020;20:1036–40.
Vermeulen M, van Schalkwyk C, Jacobs G, van den Berg K, Stone M, Bakkour S, et al. The impact of early antiretroviral treatment (ART) for HIV on the sensitivity of the latest generation of blood screening and point of care assays. Viruses. 2022;14:1426.
Fatti G, Grimwood A, Nachega JB, Nelson JA, LaSorda K, van Zyl G, et al. Better Virological outcomes among people living with human immunodeficiency virus (HIV) initiating early antiretroviral treatment (CD4 counts ≥500 cells/μL) in the HIV prevention trials network 071 (PopART) trial in South Africa. Clin Infect Dis. 2020;70:395–403.
Ye L, Chen M, Zhou X, Li Y, Liang S, Zhang Y, et al. Analysis of antiviral treatment and drug resistance among HIV/AIDS patients in Liangshan prefecture from 2016-2019. J Prev Med Intell. 2021;37:911–6+23.
Luo SL, Wang SD, Wang Y, Lin ZL, Wang KY, Zhang J, et al. Analysis of HIV antiviral treatment and drug resistance in Dazhou City, Sichuan Province, 2016-2018. J Prev Med Intell. 2021;37:634–42.
Su L, Hou X, Yuan D, Li J, Ye L, Yang H, et al. Analysis of HIV-1 drug resistance in Guangyuan city, Sichuan Province, 2012-2016. J Prev Med Intell. 2018;34:1237–41.
Liu H, Ma Y, Su Y, Smith MK, Liu Y, Jin Y, et al. Emerging trends of HIV drug resistance in Chinese HIV-infected patients receiving first-line highly active antiretroviral therapy: a systematic review and meta-analysis. Clin Infect Dis. 2014;59:1495–502.
Zhang HR, Feng YC, Dong YW, Men K. A study on the knowledge rate of AIDS among different groups in a district of Xi’an. Chin Sex Sci. 2022;31:133–7.
Bareng OT, Moyo S, Zahralban-Steele M, Maruapula D, Ditlhako T, Mokaleng B, et al. HIV-1 drug resistance mutations among individuals with low-level viraemia while taking combination ART in Botswana. J Antimicrob Chemother. 2022;77:1385–95.
Cousins S. Progress towards 2030 UN goal to end HIV epidemic falters. BMJ. 2016;354:i4025.
Acknowledgements
The authors would like to thank the Affiliated Hospital of North Sichuan Medical College, Meigu County People’s Hospital,and Sichuan Center for Disease Control and Prevention to support this study.
Funding
This research was funded by the Nanchong city school science and technology strategic cooperation special funds(19SXHZ0142); Special research project of Sichuan Medical Association Gastrointestinal Endoscopy Special Committee(2021XHNJ05).
Author information
Authors and Affiliations
Contributions
Hui Sun, Li Yuan had taken a principal role in the conception of ideas, writing the protocol, developing methodologies, analyses and write up of the article and drafted the manuscript. Kaiyou Chen contributed to the proposal writing and made a critical revision to the paper and manuscript. Yuanfang Cai, Zhonghui Zhou, Ju Yang, Wuti Jiqu, Qirong Zhu, Hong Zhang contributed to the write up of the study protocol and made revision to the paper. Shaowei Niu made revision to the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All subjects voluntarily participated in our study and signed informed consent forms before enrollment. The study protocol was approved by the Medical Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (2023ER196–1), and the study was carried out following the Helsinki Declaration of 1964.
Consent for publication
Not application.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yuan, L., Chen, K., Cai, Y. et al. Analysis of ART effects and drug resistance in adult HIV/AIDS patients in Meigu County, Liangshan Prefecture, China. BMC Infect Dis 24, 155 (2024). https://doi.org/10.1186/s12879-024-09048-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09048-y