
Abstract
Background
A lack of health resources is a common problem after the outbreak of infectious diseases, and resource optimization is an important means to solve the lack of prevention and control capacity caused by resource constraints. This study systematically evaluated the similarities and differences in the application of coronavirus disease (COVID-19) resource allocation models and analyzed the effects of different optimal resource allocations on epidemic control.
Methods
A systematic literature search was conducted of CNKI, WanFang, VIP, CBD, PubMed, Web of Science, Scopus and Embase for articles published from January 1, 2019, through November 23, 2023. Two reviewers independently evaluated the quality of the included studies, extracted and cross-checked the data. Moreover, publication bias and sensitivity analysis were evaluated.
Results
A total of 22 articles were included for systematic review; in the application of optimal allocation models, 59.09% of the studies used propagation dynamics models to simulate the allocation of various resources, and some scholars also used mathematical optimization functions (36.36%) and machine learning algorithms (31.82%) to solve the problem of resource allocation; the results of the systematic review show that differential equation modeling was more considered when testing resources optimization, the optimization function or machine learning algorithm were mostly used to optimize the bed resources; the meta-analysis results showed that the epidemic trend was obviously effectively controlled through the optimal allocation of resources, and the average control efficiency was 0.38(95%CI 0.25–0.51); Subgroup analysis revealed that the average control efficiency from high to low was health specialists 0.48(95%CI 0.37–0.59), vaccines 0.47(95%CI 0.11–0.82), testing 0.38(95%CI 0.19–0.57), personal protective equipment (PPE) 0.38(95%CI 0.06–0.70), beds 0.34(95%CI 0.14–0.53), medicines and equipment for treatment 0.32(95%CI 0.12–0.51); Funnel plots and Egger’s test showed no publication bias, and sensitivity analysis suggested robust results.
Conclusion
When the data are insufficient and the simulation time is short, the researchers mostly use the constructor for research; When the data are relatively sufficient and the simulation time is long, researchers choose differential equations or machine learning algorithms for research. In addition, our study showed that control efficiency is an important indicator to evaluate the effectiveness of epidemic prevention and control. Through the optimization of medical staff and vaccine allocation, greater prevention and control effects can be achieved.
Similar content being viewed by others

Introduction
The coronavirus disease (COVID-19) pandemic has had a profound impact on the development of the global economy and social life [1]. The epidemic has had an enormous impact on the global medical system [2]. The mortality rate of COVID-19 patients with weakened immunity is as high as 41.7%, and the mortality rate will be even worse if medical resources are insufficient [3]. In the United States, a lack of vaccine resources that prevented older adults from receiving booster doses would have resulted in US $6.7 million in direct health care costs and 3.7 quality-adjusted life-years lost over 180 days [4]. Similarly, in Brazil, one of the low- and middle-income countries with severe COVID-19 infection, patients could not receive timely treatment due to insufficient ICU beds, resulting in a mortality rate as high as 34.42% [5]. Therefore, the shortage of medical resources is an important obstacle to the prevention and control of infectious diseases.
Studies have shown that resource optimization can effectively avoid infection caused by resource constraints [6]. In previous studies on resource optimization, through retrospective cohort analysis, researchers collected the characteristics of COVID-19 infection, summarized historical experience, and provided references for resource optimization for possible future situations [7, 8]. Some scholars use some management methods, such as 6S and PDCA, to optimize the work system or process to achieve the purpose of rational allocation of resources [9]. These methods can solve the problem of resource shortages in the short term and with a small scope, and there is a time lag. However, emergent infectious diseases are characterized by a wide range of diseases and a long duration. In contrast, modeling to solve the resource optimization problem has certain advantages, which can quickly simulate the effect of resource optimization in various situations and is not limited by time and region.
The model used in resource optimization is also controversial. Seyed Ali Rakhshan et al. [10] suggested that machine learning methods are more accurate than transmission dynamics models for long-term predictions. However, the results from a study in Korea showed that transmission dynamics were more accurate than machine learning models [11]. Alaleh Azhir et al. also showed differences in the prediction effect of next-day mortality using three machine learning models [12]. The current systematic reviews mainly focus on the infection characteristics of susceptible populations [13, 14] and rarely consider the optimal allocation of resources. However, it is not clear how much effect different types of resource optimization can achieve. Therefore, this study aimed to sort out and analyze the related research on SARS-CoV-2 optimization models and evaluate the quality of research articles in this field. We systematically sorted out the application status and existing problems of the optimization model in COVID-19 resource allocation, and provided experience for formulating resource allocation plans for public health emergencies in the future.
Materials and methods
Search strategy
We searched the CNKI, WanFang, VIP, CBD, PubMed, Web of Science, Scopus and Embase databases to collect different types of SARS-CoV-2 resource allocation models. The search time limit was from January 1, 2019 to June 1, 2023.We used a combination of subject words and free words for retrieval. The search terms included: COVID-19 pneumonia, COVID-19, model, resource allocation, resource optimization, optimal control, epidemic control, etc. (Supplementary Table 1). The review protocol was registered in PROSPERO (CRD42023458855).
Literature screening
Two reviewers independently screened the studies, extracted and cross-checked the data. If there were disagreements, they were resolved by discussion or consultation with a third author. Studies were included if they (1) were related to the SARS-CoV-2 resource allocation scheme; (2) used at least one allocation model; or (3) involved optimization simulation or data simulation. The strategies that only considered the optimization of epidemic control or strategy without specific resource allocation were excluded.
Data extraction and bias assessment
The following data were extracted independently by two reviewers: general study information (authors, year of publication, country, study design, modeling methodology, outcomes of achieving objectives and resource optimization, etc.).
All the studies included in this paper were model studies. The ISPOR-SMDM task force, as a model-centered evaluation tool, not only includes the evaluation of the model itself, but also includes the evaluation of the statement of the problem, modeling purpose, and data type, which can well evaluate the quality of model studies [15].Tadele Girum et al. [16] also used the ISPOR-SMDM task force to evaluate the quality of modeling studies. Two reviewers screened items from the ISPOR-SMDM task force and assessed the quality of each study independently, including research problem description, problem transformation into modeling structure, parameter settings, resource types described, sensitivity analysis, and more (Supplementary Table 2). If the content of the included articles met the evaluation items, the evaluation was “yes”; otherwise, the evaluation was “no”, and the quality of the article was finally judged by the frequency of “yes or no”.
Statistic analysis
The average control efficiency (ACE) formula was used to obtain the comprehensive index reflecting the optimization effect [17]. The formula is as follows:
In this formulation, C is the control value of the unoptimized resource allocation. O is the control value of the optimized resource allocation.
Funnel plot analysis of publication bias was performed by Review Manager 5.3 software, and sensitivity analysis was performed by STATA 17.0 software. P < 0.05 was considered statistically significant [18, 19].
Results
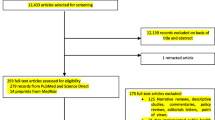
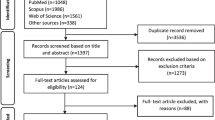
A total of 716 relevant articles were obtained. After rechecking and reading titles and abstracts, only 132 articles were screened for full text, and 22 article were finally included in the systematic review (Fig. 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the studies included in the current meta-analysis
Among the 22 articles on resource allocation, 13 articles constructed differential equation models to achieve resource allocation. It is considered that a single optimal allocation model may have some limitations in allocating resources. Therefore, 4 articles utilized a combination of two or more methods for resource allocation (Table 1).
Results of article quality evaluation
Most of the studies met the conditions for the application of the model, but 59.09% of the articles did not perform sensitivity analysis, which is an important indicator to determine the accuracy of the model. In addition, 54.55% of the studies did not provide parameter settings, initial value tables or related accessory materials, which could not be verified by other scholars through the original data (Supplementary Table 3 and Fig. 1).
Applicability analysis of the resource allocation optimization model
There are several prerequisites in model construction and resource allocation (Table 2). First, it is necessary to consider whether the data can provide the parameters of the model. In the large amount of available information and data, it is difficult to quantify the dynamic variables. Among the 22 studies included in this study, 4 studies used numerical simulation to study the problem of resource allocation. Therefore, appropriate methods could be selected to solve the problem of resource allocation. Second, suitable models were selected for the allocation of different resource types. From the included literature, differential equation modeling was more considered more when testing resource optimization. The optimization function or machine learning algorithm was mostly used to optimize the bed resources. Finally, the appropriate model is selected for implementation according to the optimization goal formulated in the study. The optimization goal can be divided into two situations: first, the maximization goal, such as resource coverage and efficiency, and second, the minimization goal, such as the prevention and control cost and demand.
Meta-analysis of control efficiency in resource allocation optimization
A total of 22 articles were included to calculate the control efficiency. According to the combined effect analysis, the epidemic trend was obviously effectively controlled through the optimal allocation of resources, and the average control efficiency was 0.38 (95% CI 0.25–0.51; I2 = 98%, P < 0.01) (Fig. 2).

Forest plot of the average control efficiency in resource optimization
According to the type of resources allocated, it was divided into different subgroups. The average control efficiency from high to low was health specialists 0.48 (95% CI 0.37–0.59; I2 = 0%, P < 0.01), vaccines 0.47 (95% CI 0.11–0.82; I2 = 98%, P = 0.01), tests 0.38 (95% CI 0.19–0.57; I2 = 86%, P < 0.01), personal protective equipment (PPE) 0.38 (95% CI 0.06–0.70; I2 = 94%, P = 0.02), beds 0.34 (95% CI 0.14–0.53; I2 = 94%, P < 0.01), medicines and equipment for treatment 0.32 (95% CI 0.12–0.51; I2 = 78%, P < 0.01)proved that comprehensive
(Fig. 3).

Results of subgroup analysis
Publication bias and sensitivity analysis
The funnel plot results were basically symmetric, suggesting a possible minor publication bias (Supplementary Fig. 2). In addition, we used Egger’s test to verify the results and found that there was no publication bias (P = 0.7119).
Sensitivity analysis showed robust results (Supplementary Fig. 3).
Discussion
In resource-constrained areas, resource optimization for infectious disease prevention and control urgently needs to be addressed. Most researchers use modeling studies to solve resource optimization problems [42, 43]. However, due to the differences in the models constructed, the resources allocated and the outcome indicators selected, the effects that can be achieved after resource optimization are also different. The systematic review and meta-analysis of the current model studies on optimizing resource allocation highlighted the importance of optimization objectives, optimization tools, and optimization resource types to evaluate and improve the efficiency of COVID-19 control. By systematically combing the articles applying the resource optimization model, we put forward the key issues that should be considered in modeling research and discussed the effect of optimizing resources.
Currently, to compare the accuracy of models, the same data are mostly used to use different models for simulation [44]. However, due to the inconsistent application conditions of different models, the data types used have a great impact on them. Meanwhile, the quality evaluation results of our included articles showed that the models rarely provided parameter settings and sources of values. The reliability of models will directly affect the formulation of optimization strategies, therefore, researchers need to understand the applicability of the model [45]. We divided the models used in the included literature into three types of resource allocation models according to their basic principles. Among them, the transmission dynamics model had at least three differential equations, which needed many parameters. Generally, the number of infections was estimated by iterative and summation methods. A study from Cameroon used a transmission dynamics model with 9 differential equations and 25 parameters to assess the impact of an intervention on transmission [46]. The optimization function requires fewer restrictions, which is suitable for less information. It is mainly constructed according to the purpose of the author, and there is no fixed framework, such as limit formula and expectation formula. A study in Brazil used three parameters to construct a model to simulate different control strategies and their cost-benefit analyses [47]. The machine learning algorithm mainly considers the impact of time on infectious diseases and is preferred when the prediction time is longer. This was also confirmed by the results of Dairi A et al. [48].
Control efficiency is an important indicator to evaluate the effectiveness of epidemic prevention and control. Xinru Wan et al. [49] used the control efficiency to reflect the transmission of SARS-CoV-2 under different temperatures and humidities. A Korean study explored the attitudes and work stress of school nurses to improve the efficiency of school infection control [50]. Resource optimization played an enormous role in the effect of epidemic control, especially when resources were limited. The results of our meta-analysis showed that the epidemic trend of COVID-19 had been effectively controlled through the optimal allocation of resources, with an average control efficiency of 0.38 (95% CI 0.25–0.51). Lin Xie et al. [51] explored the relationship between medical resources and the mortality of COVID-19 patients in Hubei Province, and found that the number of hospital beds, the number of beds in the health care system, and the number of medical staff in a unit with confirmed cases all had a significant negative impact. This is consistent with the results of this study. Resource optimization plays a role in controlling other infectious diseases. Studies by some scholars have shown that through resource optimization, AIDS, influenza A and other infectious diseases can also be rapidly controlled [52, 53]. In addition, the subgroup analysis of this study showed that the optimization of human resources, vaccine resources, testing resources and personal protection resources could achieve greater prevention and control effects, which may be related to the importance of various resources in prevention and control, but also indirectly reflects the difficulty of improving different prevention and control resources. A study in Morocco showed that the local government made various efforts to control the outbreak but lacked human resources, especially qualified human resources in intensive care and resuscitation [54]. There are differences in epidemic prevention strategies in different countries, the amount of resources is not consistent, and there are different resistances in the optimization process. However, the optimization of any type of medical resource can reduce the number of infections. Xia Wang et al. [55] also proved that comprehensive improvement of resource allocation ability can effectively reduce the infection rate.
Study limitations
Our study included 22 articles on resource optimization models, but there are still some limitations. First, due to language limitations, only Chinese and English studies were included in the study, and there may be selection bias in the selection of included studies. Second, there is a certain heterogeneity in the included literature, which is not only related to the subgroup analysis of resource type, but also related to the modeling method selected by the researchers, data time period, outcome indicators and other factors. Further research can be carried out in subgroups. Third, the meta-analysis method of the single group rate was used in this paper, which makes it difficult to control for heterogeneity, and it needs to be further confirmed by other methods. Finally, only the resource type of the included literature was classified and analyzed, but there were many other resources that were not further analyzed.
Conclusions
When the data are insufficient and the simulation time is short, the researchers mostly use the constructor for research; when the data are relatively sufficient and the simulation time is long, researchers choose differential equations or machine learning algorithms for research. In addition, our study showed that control efficiency is an important indicator to evaluate the effectiveness of epidemic prevention and control. Through the optimization of medical staff and vaccine allocation, greater prevention and control effects can be achieved. However, subsequent research should focus on improving the quality of research, improving the accuracy of the model, and establishing a simulation model that is closer to the real world.
Availability of data and materiels
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Pashaei Z, et al. Prenatal and neonatal complications of COVID-19: a systematic review. Health Sci Rep. 2022;5(2):e510.
Lobo SM, et al. Perceptions of critical care shortages, resource use, and provider well-being during the COVID-19 pandemic: a survey of 1,985 health care providers in Brazil. Chest. 2022;161(6):1526–42.
SeyedAlinaghi S, et al. COVID-19 mortality in patients with immunodeficiency and its predictors: a systematic review. Eur J Med Res. 2022;27(1):195.
Li REA. Cost-effectiveness analysis of BNT162b2 COVID-19 booster vaccination in the United States. Int j infect diseases. 2022;119(2022):87–94.
Ranzani OT, et al. Characterisation of the first 250,000 hospital admissions for COVID-19 in Brazil: a retrospective analysis of nationwide data. Lancet Respir Med. 2021;9(4):407–18.
Ren J, et al. Optimal resource allocation with spatiotemporal transmission discovery for effective disease control. Infect Dis Poverty. 2022;11(1):34.
Zahran TE, et al. Outcomes of critically ill COVID-19 patients boarding in the emergency department of a tertiary care center in a developing country: a retrospective cohort study. Int J Emerg Med. 2023;16(1):73.
Cedano J, et al. Characteristics and outcomes of patients with COVID-19 in an intensive care unit of a community hospital; retrospective cohort study. J Community Hosp Intern Med Perspect. 2021;11(1):27–32.
Wei W, et al. The application of 6S and PDCA management strategies in the nursing of COVID-19 patients. Crit Care. 2020;24(1):443.
Rakhshan SA, et al. Global analysis and prediction scenario of infectious outbreaks by recurrent dynamic model and machine learning models: a case study on COVID-19. Comput Biol Med. 2023;158:106817.
Goo T, et al. Forecasting of the COVID-19 pandemic situation of Korea. Genomics Inform. 2021;19(1):e11.
Azhir A, et al. Using shapes of COVID-19 positive patient-specific trajectories for mortality prediction. AMIA Jt Summits Transl Sci Proc. 2022;2022:130–9.
Mehraeen E, et al. COVID-19 in pediatrics: a systematic review of current knowledge and practice. Infect Disord Drug Target. 2022;22(5):e290921196908.
Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis. 2021;21(1):855.
Caro JJ, et al. Modeling good research practices--overview: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Med Decis Mak. 2012;32(5):667–77.
Girum T, et al. Optimal strategies for COVID-19 prevention from global evidence achieved through social distancing, stay at home, travel restriction and lockdown: a systematic review. Arch Public Health. 2021;79(1):150.
Cheng C, Wan X, Zhang Z. Modeling analysis reveals the transmission trend of COVID-19 and control efficiency of human intervention. BMC Infect Dis. 2021;21(1):849.
König H, König HH, Konnopka A. The excess costs of depression: a systematic review and meta-analysis. Epidemiol Psychiatr Sci. 2019;29:e30.
Alimohamadi Y, Taghdir M, Sepandi M. Estimate of the basic reproduction number for COVID-19: a systematic review and Meta-analysis. J Prev Med Pub Health. 2020;53(3):151–7.
Schmidt F, et al. Tackling the waves of COVID-19: a planning model for Intrahospital resource allocation. Front Health Serv. 2021;2021(1):718668.
Evans MV, et al. Socio-demographic variables can guide prioritized testing strategies for epidemic control in resource-limited contexts. J Infect Dis. 2023;228(9):1189–97.
Zong K, Luo CC. Reinforcement learning based framework for COVID-19 resource allocation. Comput Ind Eng. 2022;2022(167):107960.
Xue B, et al. Multi-horizon predictive models for guiding extracorporeal resource allocation in critically ill COVID-19 patients. J Am Med Inform Assoc. 2023;30(4):656–67.
Apornak A. Human resources allocation in the hospital emergency department during COVID-19 pandemic. Int J Healthcare Manag. 2021;14(1):264–70.
Arunmozhi M, et al. Managing the resource allocation for the COVID-19 pandemic in healthcare institutions: a pluralistic perspective. Int J Qual Reliab Manag. 2022;39(9):2184–204.
Chatzimanolakis M, et al. Optimal allocation of limited test resources for the quantification of COVID-19 infections. Swiss Med Wkly. 2020;2020(150):w20445.
Wang WB, Xia ZY. Study of COVID-19 epidemic control capability and emergency management strategy based on optimized SEIR model. Mathematics. 2023;11(2):323.
Libin P, et al. Assessing the feasibility and effectiveness of household-pooled universal testing to control COVID-19 epidemics. PLoS Comput Biol. 2021;17(3):e1008688.
Kim D, et al. Resource allocation for different types of vaccines against COVID-19: tradeoffs and synergies between efficacy and reach. Vaccine. 2021;39(47):6876–82.
Wang L, et al. A time-series feature-based recursive classification model to optimize treatment strategies for improving outcomes and resource allocations of COVID-19 patients. Ieee J Biomed Health Inform. 2022;26(7):3323–9.
Khan AA, Ullah S, Amin R. Optimal control analysis of COVID-19 vaccine epidemic model: a case study. Europ Phys J Plus. 2022;137(1):156.
Zhu J, Wang Q, Huang M. Optimizing two-dose vaccine resource allocation to combat a pandemic in the context of limited supply: the case of COVID-19. Front Pub Health. 2023;2023(11):1129183.
Worby CJ, Chang HH. Face mask use in the general population and optimal resource allocation during the COVID-19 pandemic. Nat Commun. 2020;11(1):4049.
Zeng L, et al. Quantitative assessment of the effects of resource optimization and ICU admission policy on COVID-19 mortalities. Phys Rev Res. 2022;4(3):033209.
Mehrotra S, et al. A model of supply-chain decisions for resource sharing with an application to ventilator allocation to combat COVID-19. Nav Res Logist. 2020;67(5):303–20.
Majid A, et al. A two-stages mathematical model for a Covid-19 vaccination fuzzy scheme and resource allocation in hub locations considering transmission risk and environment factor. Rairo-Operat Res. 2023;57(3):1097–123.
Barnieh L, et al. Remdesivir for hospitalized COVID-19 patients in the United States: optimization of health care resources. Infect Dis Ther. 2023;12(6):1655–65.
Kim J, et al. Optimal triage for COVID-19 patients under limited health care resources with a parsimonious machine learning prediction model and threshold optimization using discrete-event simulation: development study. JMIR Med Inform. 2021;9(11):e32726.
Lam SSW, et al. An agile systems modeling framework for bed resource planning during COVID-19 pandemic in Singapore. Front Pub Health. 2022;2022(10):714092.
Zhou D, et al. EPH172 when is it valuable for COVID-19 booster dose?: a transmission dynamics model-based effectiveness and cost-effectiveness analysis of two booster dose vaccination priority strategies in mainland China. Value Health. 2022;25(7):S466.
Reddy KP, et al. Clinical outcomes and cost-effectiveness of COVID-19 vaccination in South Africa. Nat Commun. 2021;12(1):6238.
Aydin N, Cetinkale Z. Analyses on ICU and non-ICU capacity of government hospitals during the COVID-19 outbreak via multi-objective linear programming: an evidence from Istanbul. Comput Biol Med. 2022;2022(146):105562.
Demers J, et al. The relationship between controllability, optimal testing resource allocation, and incubation-latent period mismatch as revealed by COVID-19. Infect Dis Model. 2023;8(2):514–38.
Conde-Gutiérrez RA, Colorado D, Hernández-Bautista SL. Comparison of an artificial neural network and Gompertz model for predicting the dynamics of deaths from COVID-19 in México. Nonlinear Dyn. 2021;104(4):4655–69.
Farooq J, Bazaz MA. A novel adaptive deep learning model of Covid-19 with focus on mortality reduction strategies. Chaos Solitons Fractals. 2022;2020(138):110148.
Tadmon C, Foko S. A transmission dynamics model of COVID-19: case of Cameroon. Infect Dis Model. 2022;7(2):211–49.
Omame A, et al. COVID-19 and dengue co-infection in Brazil: optimal control and cost-effectiveness analysis. Eur Phys J Plus. 2021;136(10):1090.
Dairi A, et al. Comparative study of machine learning methods for COVID-19 transmission forecasting. J Biomed Inform. 2021;2021(118):103791.
Wan X, Cheng C, Zhang Z. Transmission rate and control efficiency of COVID-19 was lower in warm and wet climate. Int J Environ Health Res. 2022:1–12.
Yim MR, Kim B. Factors affecting infection control performance of school health nurses during the COVID-19 pandemic in South Korea. J Multidiscip Healthc. 2022;15:805–14.
Xie L, et al. Medical resources and coronavirus disease (COVID-19) mortality rate: evidence and implications from Hubei province in China. PLoS One. 2021;16(1):e0244867.
Kedziora DJ, et al. Optimal allocation of HIV resources among geographical regions. BMC Pub Health. 2019;19(1):1509.
Venkatramanan S, et al. Optimizing spatial allocation of seasonal influenza vaccine under temporal constraints. PLoS Comput Biol. 2019;15(9):e1007111.
Barkia A, et al. Morocco's National Response to the COVID-19 pandemic: public health challenges and lessons learned. JMIR Public Health Surveill. 2021;7(9):e31930.
Wang X, et al. Effects of medical resource capacities and intensities of public mitigation measures on outcomes of COVID-19 outbreaks. BMC Pub Health. 2021;21(1):605.
Funding
This research was funded by the Xinjiang Production and Construction Corps Scientific and Technological Research Project (2021AB034).
Author information
Authors and Affiliations
Contributions
YYW designed the study, extracted and analyzed the data, and wrote the article. WWZ and ZXL assisted YYW in literature search and screening. JLS and MXJ contributed to the idea and design of this study, advised on analysis and revised the manuscript. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, YY., Zhang, WW., Lu, Zx. et al. Optimal resource allocation model for COVID-19: a systematic review and meta-analysis. BMC Infect Dis 24, 200 (2024). https://doi.org/10.1186/s12879-024-09007-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09007-7