
Abstract
Hand foot and mouth disease (HFMD) is caused by a variety of enteroviruses, and occurs in large outbreaks in which a small proportion of children deteriorate rapidly with cardiopulmonary failure. Determining which children are likely to deteriorate is difficult and health systems may become overloaded during outbreaks as many children require hospitalization for monitoring. Heart rate variability (HRV) may help distinguish those with more severe diseases but requires simple scalable methods to collect ECG data.
We carried out a prospective observational study to examine the feasibility of using wearable devices to measure HRV in 142 children admitted with HFMD at a children’s hospital in Vietnam. ECG data were collected in all children. HRV indices calculated were lower in those with enterovirus A71 associated HFMD compared to those with other viral pathogens.
HRV analysis collected from wearable devices is feasible in a low and middle income country (LMIC) and may help classify disease severity in HFMD.
Similar content being viewed by others

Introduction
Hand foot and mouth disease (HFMD) is caused by enteroviruses and mainly affects children under five years of age. Over the last two decades, HFMD has become a major public health concern in the Asia–Pacific region where huge outbreaks have occurred. To date, these outbreaks total more than 16,000,000 cases and 4000 deaths [1, 2]. Over recent years, major outbreaks of HFMD have occurred in Vietnam: over 200,000 children were hospitalized in 2011–12 and over 130,000 in 2018 [3]. Whilst enterovirus A71 (EV-A71) remains the dominant enterovirus associated with severe HFMD in Vietnam,, cocksackievirus A10 (CVA10), cocksackievirus A6 (CVA6), and cocksackievirus A8 (CVA8) have also been detected [3].
Whilst infections are generally asymptomatic or uncomplicated, severe disease with central nervous system (CNS) involvement occurs in a small number of cases and is particularly linked to infection with EV-A71 or CVA6. Central nervous system (CNS) complications (most commonly meningoencephalitis or brainstem encephalitis) are seen in up to 30% of hospitalized cases of EV-A71 associated HFMD [4]. Severe cases can progress rapidly to cardiopulmonary failure which is the principal cause of death from HFMD [4].
There is a close temporal relationship between neurological signs and onset of tachycardia, hypertension and pulmonary oedema in those with severe disease. Magnetic resonance imaging (MRI) features, mainly studied in EV-A71 disease, show inflammation in the grey matter in the spinal cord, hypothalamus and medulla oblongata, including the dorsal nucleus of the vagus nerve [2, 5]. Consequently, it is hypothesized that cardiorespiratory complications of severe HFMD are linked to autonomic nervous system dysregulation resulting from CNS damage [2].
Clinical features suggestive of autonomic nervous system activation may be early indicators of those at risk of progression to severe diseases [6]. Nevertheless, these features lack specificity limiting their use, particularly in outbreak situations. Heart rate variability (HRV), is an alternative indicator of autonomic nervous system activity. HRV parameters are derived from statistical analysis of beat-to-beat variation in the heart rate. From these, inferences are drawn regarding the activity of the autonomic nervous system, normally responsible for control of heart rate (Supplementary Table 1) [7]. In a study of 46 Taiwanese children with clinical signs of HFMD and herpangina [8, 9], a reduction in HRV with increasing disease severity was observed. Early changes in HRV, preceding clinical signs, were observed in the 6 cases who progressed to severe disease.
Whilst promising as a tool for triage and detection of children at risk of severe disease, traditional HRV evaluation is conducted retrospectively from Holter monitor ECG recordings. Not only is this cumbersome in the small children in whom most HFMD occurs, but it is also unsuitable for real-time analysis needed in for clinical utility. The advent of light-weight wearable ECG monitors raises the possibility of using such devices to evaluate HRV changes in real-time [10, 11]. Such systems, in theory, are ideally suited for outbreak situations in low-resource settings as many are low-cost and potentially scalable, but the feasibility of this approach has yet to be established [12].
The aim of this study was to pilot the use of low-cost wearable devices to record ECG in children with HFMD, evaluating feasibility of use as well as describing HRV characteristics related to the underlying viral aetiology and clinical severity.
Methods
The study was conducted at the Children’s Hospital 1, a tertiary care center located in Ho Chi Minh City which provides child’s health services for children up to 16 years old in Southern Vietnam. Hospitalized patients aged 16 years old or younger, with a clinical diagnosis of HFMD of Grades 2a to grade 4 (Table 1 [13]) during the first 7 days of illness were eligible for enrollment. Patients’ legal representatives gave written informed consent before patients were enrolled. As this was a pilot study, a pragmatic sample size of at least 120 patients was calculated in order to include at least 30 very severe patients (Grade 3 or 4) [14].
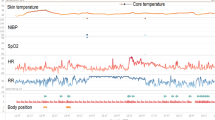
ECG signal was collected for up to 24 h, using e-Patch (DELTA Danish Electronics) wearable ECG monitor (See Supplementary Fig. 1). Patient’s clinical and demographic data were collected at enrolment and patients followed until hospital discharge. Throat swabs were collected from all participants at enrolment in order to identify pathogens using PCR methods previously described [3]. Normal values for heart rate are given in Supplementary Box 1.
HRV analysis was performed after manually editing of ECG to exclude noise and artefacts. Recordings were divided into 5-min windows. All 5-min windows with artefacts or noise were excluded. The remaining recordings were analyzed using the sequential function of HRV analysis software version 1.1 (St. Etienne University, France [15]). For severe and very severe patients (Grades 2b, 3 and 4) who were admitted to the Emergence Room or Intensive Care Unit, the mean HRV indices derived from night time windows (between 10 pm to 4 am) were used for analysis as these were likely to be times of maximum quiet. For children with mild grades who were observed in other wards, recording durations were approximately six hours during day-time. For these patients, means of HRV indices from three consecutive five-minute HRV windows when patients were calm (based on regularity of heart rates) were used.
HRV indices were calculated with the reference being standard and a re-sampling rate of 2 Hz. HRV was analyzed using time domain, frequency domain and non-linear (Poincaré plot analysis) approaches [16]. The HRV indices selected are defined in Supplementary Table 1 and were selected as most commonly used and those recommended by consensus guidelines.
Median and inter quartile range (IQR) are given for skewed variables. Statistical differences in HRV indices among severities of disease and groups of detected pathogens were tested using the Mann–Whitney U- test. Corrections were not made for multiple testing.
Results
From April 2017 to December 2018, 142 patients were enrolled in the study. Of these, the numbers of children with grade 2a, 2b1, 2b2, grade 3 and grade 4 were 40 (28.2%), 16 (11.3%), 32 (22.5%), 50 (35.2%) and 4 (2.8%) respectively. Demographic characteristics and clinical features at enrollment are described in Table 2. Almost all cases (97.2%) were younger than 60 months with a median age of 21.7 (IQR: 2.4–154.8) months. Of the patients enrolled, 34 (23.9%) were treated with phenobarbital, 2 (2.1%) with vasopressors/inotropes and 33 (23.2%) with milrinone as per Ministry of Health guidelines [13]. Two patients required mechanical ventilation and all patients survived to hospital discharge.
In all patients, ECG signal was obtained and no adverse events associated with the wearable occurred. A total of 5526 5-min ECG recordings were available for analysis. Of these, 120 segments were from patients with grade 2a disease, 863 from grade 2b1, 1783 from 2b2, 2627 from grade 3 and 133 from children with grade 4 disease.
Clinical features on admission are given in Table 2. As may be expected, clinical presentation, the proportion of high fever, lethargy, myoclonus, trembling and mottled skin in severe and very severe group were more prominent than in the mild group. The most common enterovirus serotype was EV-A71 80/142 (56.3% of cases). In the severe and very severe group, 68/102 (66.7%) children had EV-A71 detected. Conversely, CVA6, CVA10 and CVA16 were more common in those with mild disease (Table 2).
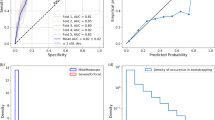
HRV data are presented in Figs. 1 and 2 and Supplementary Tables 2 and 3. When comparing HRV parameters according to pathogen, HRV parameters in those with EVA-71 associated disease were consistently lower across and severities (Figs. 1 and 2). Those parameters associated with overall ANSD activity shown in Fig. 1 show a trend of reduced measured variability in more mild disease (Supplementary Table 3). Specifically looking at variability parameters linked to ANSD activity and balance (Fig. 2), high frequency (HF) variability which is associated with vagal activity is lower with increasing disease severity, particularly in EVA-71 disease. The opposite pattern is seen with low frequency (LF) measurements, generally accepted to represent a combination of sympathetic and parasympathetic activity. SD1 and SD2 values (indicating parasympathetic and parasympathetic/sympathetic activity respectively) are lower in EVA-71 patients but trends related to disease severity are less clear.

HRV indices according to both disease severity and pathogen. Figure shows HRV indices according to pathogen (EVA-71 red, other viruses green) and severity of disease. Mild (2a), Severe (2b1), very severe (2b2, 3 & 4). Panels: left Total power (ms.2); right Standard deviation of NN intervals -SDNN (ms)

Distribution of HRV indices reflecting the general activity of ANS by pathogens in different severities. Figure shows HRV indices according to pathogen (EVA-71 red, other viruses green) and severity of disease. Mild (Grade 2a), Severe (Grades 2b1& 2b2) very severe (Grades 3 & 4). Panels above-below from left to right: High Frequency (HF) (ms2); High frequency normalized units (HFnu) (%); Low Frequency (LF) (ms.2); Low Frequency normalized units (LFnu) (%); SD1 (ms); SD1 normalizised units (%); SD2 (%); SD2 (ms); SD2 normalized units (%)
Discussion
We have demonstrated the feasibility of continuous ECG monitoring using wearable devices in young children with HFMD. Unlike traditional methods of wired monitoring or Holter ECG monitoring, wearable devices offer the ability to monitor patients of varying disease severity using a single device. The device we chose has the advantage of being a two-part system with a re-usable sensor connected to a disposable single-use electrode and is thus particularly suited for use in resource-constrained settings.
Interpreting HRV in detail in this study is complex due to the observational nature of our study and complex nature of cardiovascular control itself. Nevertheless, our findings regarding HRV values are consistent with other studies demonstrating lower values than healthy children and a relationship with disease severity [9, 17, 18]. We did not include patients with Grade 1 disease as these patients are not admitted to hospital and a future study may also include this group. Unlike previously reported HRV data for HFMD, we have been able to describe HRV according to specific pathogen and have demonstrated reduced HRV with EVA-71 associated disease, supporting clinical and imaging findings that EVA-71 is associated with most severe disease and CNS involvement [1].
The HRV metrics we present include a mixture of time, frequency and non-linear evaluations of beat-to-beat heart rate variation occurring in 5-min segments. Our data show reassuring internal consistency between time, frequency and non-linear measures. Clinical interpretation of individual indices, however, is complex. Clearest evidence supports interpretation of high-frequency HRV as representing vagal activity whereas other measures include more complex interactions between parasympathetic, sympathetic and vasomotor reflexes [8]. Nevertheless, a general interpretation of our data suggest a relative increase in sympathetic activity compared to parasympathetic and a reduction in parasympathetic activity in more severe disease or disease with EVA-71. A similar conclusion was made by authors of the study in Taiwanese children and is supported by MRI data of medulla oblongata involvement [2, 19].
Given the complex nature of HRV and the pragmatic nature of our pilot study, we caution over-interpretation of our data. HRV can be affected by eating, exercise, emotional state and drugs, all of which may be different between the groups in our study. Furthermore, more severe cases remained in hospital for longer periods giving rise to further possible bias in our results. By using only 5-min segments, we achieved a consistent length window for HRV analysis as window duration can significantly affect some indices. Data from a larger sample may allow better control for confounding factors and we believe that wearable devices may offer a suitable collection method for further data. With appropriate technology, data can be fed into near real-time decision support tools and assist in prognostic models for clinical care and triage. Currently there are still limited platforms and software available for such prognostication, especially in LMICs. In parallel with this project, we have created an open-source signal quality control tool and are working with a local partner to create a scalable real-time platform. However such initiatives are rare and without appropriate support from commercial partners or funders, innovative technologies are at risk of being developed only for high-income settings and problems [20,21,22,23,24].
Conclusions
Our overall aim in this study was to pilot the use of wearables and gain some insight into pathogen differences in HRV. Our results indicate that wearable monitors are feasible in young children in a LMIC setting and that there are differences in HRV related to disease aetiology. These differences could potentially be incorporated into prognostic models to aid triage in outbreak situations.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Nguyen NTB, Pham HV, Hoang CQ, Nguyen TM, Nguyen LT, Phan HC, et al. Epidemiological and clinical characteristics of children who died from hand, foot and mouth disease in Vietnam, 2011. BMC Infect Dis. 2014;14(1):341.
Solomon T, Lewthwaite P, Perera D, Cardosa MJ, McMinn P, Ooi MH. Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect Dis. 2010;10(11):778–90.
Nhan LNT, Hong NTT, Nhu LNT, Nguyet LA, Ny NTH, Thanh TT. Severe enterovirus A71 associated hand, foot and mouth disease, Vietnam, 2018: preliminary report of an impending outbreak. Euro Surveill. 2019;23(46):1800590.
WHO W. A guide to clinical management and public health response for hand, foot and mouth disease (HFMD). 2011.
Lian ZY, Li HH, Zhang B, Dong YH, Deng WX, Liu J, et al. Neuro-magnetic resonance imaging in hand, foot, and mouth disease: finding in 412 patients and prognostic features. J Comput Assist Tomogr. 2017;41(6):861–7.
Hoang MTV, Nguyen TA, Tran TT, Vu TTH, Le NTN, Nguyen THN, et al. Clinical and aetiological study of hand, foot and mouth disease in southern Vietnam, 2013–2015: Inpatients and outpatients. Int J Infect Dis. 2019;80:1.
Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Heal. 2017;5:1–17.
Heathers JAJ. Everything Hertz: Methodological issues in short-term frequency-domain HRV. Front Physiol. 2014;5:1–15.
Lin M-T, Wang J-K, Lu FL, Wu E-T, Yeh S-J, Lee W-L, et al. Heart rate variability monitoring in the detection of central nervous system complications in children with enterovirus infection. J Crit Care. 2006;21(3):280–6.
Ghiasi S, Zhu T, Lu P, Hagenah J, Khanh PNQ, Van HN, et al. Sepsis mortality prediction using wearable monitoring in low-middle income countries. Sensors. 2022;22(10):3866.
Lu P, Ghiasi S, Hagenah J, Hai HB, Hao N Van, Nguyen P, et al. Classification of tetanus severity in intensive-care settings for low income settings using wearable sensors. Sensors(Basel). 2022;22(17):6554. https://doi.org/10.3390/s22176554.
Ming DK, Sangkaew S, Chanh HQ, Nhat PTH, Yacoub S, Georgiou P, et al. Continuous physiological monitoring using wearable technology to inform individual management of infectious diseases, public health and outbreak responses. Int J Infect Dis. 2020;96:648–54.
Viet Nam Ministry of Health. Communicable Diseases. 2016. p. 189–90.
Arain M, Campbell MJ, Cooper CL, Lancaster GA. What is a pilot or feasibility study? BMC Med Res Methodol. 2010;10(67):1–7.
Pichot V, Roche F, Celle S, Barthélémy JC, Chouchou F. HRV analysis: A free software for analyzing cardiac autonomic activity. Front Physiol. 2016;7:1–15.
Nguyen Phu Thu T, Hernandez AI, Costet N, Patural H, Pichot V, Carrault G, et al. Improving methodology in heart rate variability analysis for the premature infants: Impact of the time length. PLoS One. 2019;14(8):e0220692. https://doi.org/10.1371/journal.pone.02.
Thi H, Duong H, Tadesse GA, Tran P, Nhat H, Van HN, et al. Heart rate variability as an indicator of autonomic nervous system disturbance in tetanus. Am J Trop Med Hyg. 2020;102(2):403–7.
Pichot V, Flori S, Giraud A, Patural H, Pichot V, Flori S, et al. Autonomic maturation from birth to 2 years: normative values. Heliyon. 2019;5(3):e01300. https://doi.org/10.1016/j.heliyon.2019.e01300.
Lin MT, Wang JK, Lu FL, Wu ET, Yeh SJ, Lee WL, et al. Heart rate variability monitoring in the detection of central nervous system complications in children with enterovirus infection. J Crit Care. 2006;21(3):280–6.
Task Force of the European Society of Caridiology and the North American Society of Pacing Electrophysiology. Hear rate variability. Circulation. 1996:1043–65.
Task Force of The European Society of Cardiology and The North American, Electrophysiology S of P and E. Guidelines Heart rate variability. Eur Heart J. 1996;17:354–81.
Pichot V, Roche F, Celle S, Barthélémy JC CF. HRVanalysis: a free software to analysis cardiac autonomic activity. Front Physiol. 2016;7:557. https://doi.org/10.3389/fphys.2016.00557.
Akemi R, Marcelo C, Carlos L, Vanderlei M, Fernandes M. Autonomic neuroscience: basic and clinical Poincaré plot indexes of heart rate variability: relationships with other nonlinear variables. Auton Neurosci Basic Clin. 2013;177(2):271–4.
Le VD, Ho HB, Karolcik S, et al. vital_sqi: A Python package for physiological signal quality control. Front Physiol. 2022;13:1020458.
Acknowledgements
Staff and children at Children’s Hospital Number 1.
John Prince.
Funding
Wellcome Trust: 204904/Z/16/Z.
DAC is funded by a Royal Academy of Engineering Research Chair, an NIHR Research Professorship, the NIHR Oxford Biomedical Research Centre, the InnoHK Centre for Cerebro-cardiovascular Engineering, and the Pandemic Sciences Institute at Oxford.
Author information
Authors and Affiliations
Contributions
NTN, CLT, HRVD and LVT conceived the study. LNTN, THK, NTTH, NTHN, LNTN, DDKH implemented the study, collecting and curated data. TTT, LVT, GAT, TTZ, DC were responsible for study methodology, NTN, TTT, carried out primary data analysis, DC, LVT, CLT, GAT, RVD THK, NTH provided supervision and oversight. LNTN, LVT, CLT and HFVD drafted the initial manuscript. All authors reviewed and agreed the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki. The study was approved by the ethical committees of Children’s Hospital Number 1 Ho Chi Minh City and Oxford Tropical Research Ethics Committee. All participants were children and written informed consent was given by their legal representatives.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Commonly used heart rate variability indices. Supplementary Box 1. Children’s Hospital 1 guidelines for normal heart rate in children within study age-groups. Supplementary Table 2. Heart rate variability indices in children with HFMD by pathogen. Definitions of HRV indices are given in Supplementary Table 1. Supplementary Table 3. HRV indices according to grade of disease. Definitions of HRV indices are given in Supplementary Table 1.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Nhan, L.N.T., Hung, N.T., Khanh, T.H. et al. Feasibility of wearable monitors to detect heart rate variability in children with hand, foot and mouth disease. BMC Infect Dis 24, 205 (2024). https://doi.org/10.1186/s12879-024-08994-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-08994-x