
Abstract
Background
Although Ethiopia is working towards measles elimination, a recurrent measles outbreak has occurred. To take appropriate measures, previously, many fragmented and inconsistent outbreak investigations were done, but there is no consolidated evidence on attack rate, case fatality rate, and determinants of measles infection during the measles outbreak. This systematic review and meta-analysis aimed to identify cumulative evidence on attack rate, case fatality rate, and determinants of measles infection during the outbreak.
Methods
A systematic literature review and Meta-analysis was used. We searched Google Scholar, Medline/PubMed, Cochrane/Wiley Library, EMBASE, Science Direct, and African Journals Online databases using different terms. Investigations that applied any study design, data collection- and analysis methods related to the measles outbreak investigation were included. Data were extracted in an Excel spreadsheet and imported into STATA version 17 software for meta-analysis. The I2 statistics were used to test heterogeneity, and ‘Begg’s and ‘Egger’s tests were used to assess publication bias. The odds ratio (OR) with a 95% confidence interval (CI) was presented using forest plots.
Results
Eight measles outbreak investigations with 3004 measles cases and 33 deaths were included in this study. The pooled attack rate (A.R.) and case fatality rate were 34.51/10,000 [95% CI; 21.33–47.70/10,000] population and 2.21% [95% CI; 0.07-2.08%], respectively. Subgroup analysis revealed the highest attack rate of outbreaks in the Oromia region (63.05 per 10,000 population) and the lowest in the Amhara region (17.77 per 10,000 population). Associated factors with the measles outbreak were being unvaccinated (OR = 5.96; 95% CI: 3.28–10.82) and contact history (OR = 3.90; 95% CI: 2.47–6.15).
Conclusion
Our analysis revealed compelling evidence within the outbreak descriptions, highlighting elevated attack and case fatality rates. Measles infection was notably linked to being unvaccinated and having a contact history. Strengthening routine vaccination practices and enhancing contact tracing measures are vital strategies moving forward.
Similar content being viewed by others


Introduction
A measles outbreak investigation is the diagnosis and confirmation of a suspected measles outbreak through the urgent and intelligent use of appropriate procedures to take suitable measures toward controlling the outbreak [1, 2]. The purposes of measles outbreak investigation are to assess the extent of the outbreak, search for additional cases, identify the source of the epidemic and the population at risk, and institute timely case management to reduce morbidity and mortality and prevent future attacks [1,2,3].
Measles is the most contagious viral human disease, commonly resulting in wide-ranging outbreaks [4, 5]. Any person with fever, maculopapular rash, cough, coryza/runny nose, or conjunctivitis/ red eyes is a suspect of a measles case. When the suspect measles case is positive for an immunoglobulin M (IgM) antibody test, it is called a confirmed measles case [3, 4]. Measles is transmitted through droplets from nose, mouth, or throat secretions [6]. It has a secondary attack rate of 90% in susceptible household and institution contacts [4, 5]. The most severe complications of measles are blindness, pneumonia, and encephalitis, leading to case fatality rates ranging from 0.1% in industrial countries to 15% in developing countries [7, 8]. Severe complications of measles are more common in children under 5 years and adults older than 20 years old [8].
A suspected measles outbreak is the occurrence of five or more reported suspected measles cases in one month per 100,000 population living in a geographic area such as a kebele, woreda, or health facility catchment area. A confirmed measles outbreak is the occurrence of three or more laboratory-confirmed suspected measles cases in one month per 100,000 population living in a geographic area such as a kebele, woreda, or health facility catchment area [9].
An outbreak occurs when the accumulated number of susceptible individuals is greater than the critical number of susceptible individuals for a given population to sustain transmission [2, 3]. Approximately 15% of children vaccinated at nine months of age and 5% of those vaccinated at 12 months of age fail to seroconvert and are thus not protected after vaccination [3].
Even though there is a significant success in global measles mortality reduction and elimination [7], more than 100,000 measles deaths occurred in 2017 [10]. More than 95% of these deaths occurred in low-income countries [11]. Although the African region and Ethiopia are working towards measles elimination by 2020 [3], Ethiopia is still the 4th top country in the world in the burden of measles cases [1].
An outbreak investigation is conducted within 3 h of notification of a suspected measles outbreak [12]. Timely outbreak investigation and response may reduce morbidity, mortality, and the spread of the outbreak [3]. It is also one of the most important measures for eliminating measles [13].
In 2019, Ethiopia introduced the measles vaccine second dose (MCV2) vaccination into the routine immunization program in the second year of life for measles elimination [10]. Despite these efforts, in Ethiopia, a recurrent measles outbreak has occurred [14].
Ethiopia initiated a field epidemiology and laboratory training program in 2009 [15]. This program has played a significant role in improving outbreak detection and investigation. There are many single, fragmented measles outbreak investigations in Ethiopia, but there is a lack of collective evidence on the attack rate, case fatality rate, and determinants of measles infection during the outbreak. Therefore, this systematic review and meta-analysis aimed to measure the attack and case fatality rates and identify measles infection determinants during the outbreak investigation.
Methods
Study design and searching methods
This investigation used a systemic review and Meta-analysis of published measles outbreak investigations. Published investigations were searched in Google Scholar, MEDLINE/PubMed, Cochrane/Wiley Library, EMBASE, Science Direct, and African Journals Online databases. The search terms used were “Measles attack rate OR Measles incidence OR Measles case fatality rate OR Measles outbreak investigation OR Measles outbreak ORMeasles epidemic OR Determinant of measles infection OR investigation of measles outbreak or Risk factors of a measles outbreak and Ethiopia.“
Investigation selection and eligibility criteria
This systematic review and meta-analysis encompassed all published studies that examined measles outbreaks in Ethiopia. The study design of the included investigations was not restricted. The review incorporated measles outbreak studies published in English between 2010 and 2022.
Outcomes
This review has outcome variables for the measles attack rate, which is calculated as the number of people who became ill from measles divided by the number of people at risk for the measles disease, and the case fatality rate, which is calculated as the number of measles-related deaths by the number of measles total cases [16]. The determinants of contracting a measles virus were also outcome variables. Vaccination status and contact were determinants of measles virus infection.
Quality assessment
The included investigations were assessed for quality, with only high-quality investigations included in the meta-analysis. Two independent authors assessed each investigation’s quality by using an adapted Newcastle- Characteristics of included investigations tool [17]. Generally, the tool consists of three sections; the first section is ranked out of five stars and reflects the methodological quality of each primary investigation. The second section compares the study outcomes or exposures with the possibility of adding two stars. The third section focuses on each primary study’s outcome and statistical analysis, with the possibility of three stars [18]. We compared the quality assessment scores of the investigations and determined any difference before computing the final assessment score. Investigations with a score of > 7 out of 10 scales were assumed to be high quality, revealing that all investigations were eligible.
Data extraction and management
Before data extraction, a standard tool was adapted by reviewing different kinds of literature. The data extraction tool included such information as Author name, publication year, journal name, publication year, study design, study period, study setting, sample size, descriptive data analysis (attack rate, case fatality rate, outbreak duration, and vaccination status), and factors of a measles outbreak. The data extraction tool was developed independently by two authors and revised by another two authors. Before data collection, all authors agreed on the tool.
Data analysis
Data was collected and organized in an Excel spreadsheet and transferred to STATA version 17 software to conduct the meta-analysis. The primary focus of the systematic review and meta-analysis was on the comprehensive assessment and consolidation of attack rates, case fatality rates, and factors influencing measles infection.
The combined attack and case fatality rates and their corresponding 95% confidence intervals (CI) were calculated by employing each study’s attack rate, case fatality rate, and standard error information. The results were visually represented through forest plots, illustrating the 95% CI for attack rates, case fatality rates, and odds ratios (OR) related to factors associated with measles virus infection.
Subgroup analysis was conducted to investigate potential disparities, considering factors such as region and study period. A random effects model was utilized in the meta-analysis to account for heterogeneity across the included studies [19].
Heterogeneity and publication bias
The investigation’s heterogeneity was tested using the I squared (I2) test statistic and its corresponding p-value [20]. A p-value less than 0.05 was used to declare heterogeneity [21]. I2 25, 50, and 75% statistics were used to declare low, moderate, and high heterogeneity, respectively [19]. ‘Egger’s and ‘Begg’s tests are commonly used to assess potential publication bias in a meta-analysis, and a p-value less than 0.005 to state its significance [22, 23].
Results
Study selection
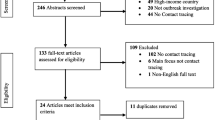
Through electronic database searches, we accessed a total of 136 records. Initial screening was done by assessing titles, abstracts, and complete article reviews, excluding 90 articles based on title and abstract evaluations. Subsequently, 30 articles underwent eligibility evaluation, with 22 being excluded due to incomplete reporting. Ultimately, 8 investigations met the criteria and were incorporated into this meta-analysis (Fig. 1).

Flow Diagram of measles outbreak investigation included in systematic review and meta-analysis in Ethiopia, 2022
Characteristics of included investigations
This systematic review and meta-analysis encompassed eight distinct investigations of measles outbreaks, involving a cumulative count of 3004 confirmed measles cases and resulting in 33 reported fatalities (age range: 1 month to 75 years) [17, 24,25,26,27,28,29,30]. More than three-fifths (62.5%) of the investigations were case-control study designs [24, 27,28,29,30], and three articles were descriptive cross-sectional study designs [17, 25, 26]. All included outbreak investigations used both primary and secondary data sources, which were investigated from 2009 to 2021. Four articles were conducted in the Amhara region [24, 25, 28, 29], three in the Oromia region [17, 27, 30], and one in the Somalia region [26] (Table 1).
Attack rate
This systemic review and meta-analysis’s pooled attack rate (A.R.) was 34. 51 (95% CI: 21.33–47.70) per 10,000 population [17, 24,25,26,27,28,29,30] (Fig. 2). Higher and more significant heterogeneity ( I2 = 97.35% and p-value < 0.000). Considerable publication bias was also detected, with Eggers, .

Pooled attack rate of measles during an outbreak in Ethiopia. p-value = 0.00047 and ‘Begg’s = 0.00053 (Fig. 2)
Case fatality rate (CFR)
The overall pooled CFR of this investigation was 2.21% (95% CI: 0.07-4.36%) [17, 25,26,27,28, 30]. There is moderate and significant heterogeneity, I2 = 70%, and a p-value of < 0.00001. Significant publication bias was also detected, Begg’s = 0.00853 and ‘Egger’s = 0.00436 (Fig. 3).

Pooled case fatality rate during the measles outbreak in Ethiopia
Subgroup analysis
Subgroup analysis of attack rate done by region showed that the highest attack rate was observed in the Oromia region, 63.05 (95% CI; 47.54–126.12) per 10,000, and the lowest in the Amhara region, 17.77 (95% CI; 5.58–29.95) per 10,000 population. A higher attack rate of measles was observed after 2019, 91.02 (95% CI; 35.17 -146.87) per 10,000 population (Table 2).
In subgroup analysis, the Amhara region, 2.83% (95% CI; 0.86-6.52%), and the Oromia region, 2.46% (95% CI; 1.77 -6.70%), had almost equal CFR. A higher case fatality rate was reported after 2019, at 3.35% (95% CI; 3.10-9.81%) (Table 3).
According to the existing evidence, vaccination status and contact history were the main determinants of measles infection.
Vaccination status
The vaccination status measured as being vaccinated or unvaccinated strongly influenced contracting the measles virus in four outbreak investigations [24, 27, 29, 30]. The meta-analysis revealed that individuals who had not been vaccinated against the measles virus were six times more likely to contract the virus (OR = 5.68; 95% CI: 4.41–6.95). The heterogeneity test showed that there is no evidence of heterogeneity (I2 = 0, and p-value = 0.99). However, there is a significant publication bias (‘Begg’s test = 0.00032 and ‘Egger’s test = 0.0043) (Fig. 4).

Pooled odds ratio between vaccination status and contracting the measles virus
Contact history
A contact history significantly affected the acquisition of the measles virus [24, 27,28,29,30]. It was identified that individuals who had a contact history with measles cases 7–21 days before developing the current infection had four times (AOR = 3.54; 95% CI: 2.02–5.05) higher risk of acquiring measles infection as compared to those individuals who had no contact history during the same period. There was a significant publication bias (‘Begg’s test = 0.0036 and ‘Egger’s test = 0.0023). However, there was no evidence of heterogeneity, I2 = 0, and p-value < 0.91 (Fig. 5).

Pooled odds ratio between contact history and contracting the measles virus
Discussion
This systematic review and meta-analysis was conducted to measure the attack and case fatality rates and identify factors associated with measles infection in Ethiopia using available published articles. The overall pooled attack rate of measles during a measles outbreak was 34.51 (95% CI: 21.33–47.70) per 10,000 population. The highest and lowest attack rates were 120 per 10,000 population [30] and 1.18 per 10,000 population [28], respectively. The variation in attack rate from outbreak to outbreak could be attributed to differences in the range of the outbreak, susceptible accumulation, and nutritional status of the population. In addition to this, there might be differences in the time of outbreak investigation and response-to-action threshold. Timely outbreak investigation and response reduce morbidity, mortality, and the spread of the outbreak [3]. In three measles outbreak investigations, the highest age-specific attack rate was reported in the age group of < 1-year-old children, which was 1.7/10,000 [17], 47.6/10,000 [29], and 310/10,000 populations [30] Immunity of children can be lost in just over 2.5 months after birth or the time breastfeeding is discontinued [31]. In two investigations, the highest age-specific attack rate was reported among the age group of 15–44 years (93.8 per 10,000) [24], and under 5 years (38/1000 population) [30]. In another investigation, the highest age-specific attack rate (291 per 10,000 population) was observed at the age of 5–14 years [28]. Variations in age-specific attack rates could be attributed to differences in the immune status. A more susceptible population could be found in these age groups.
In seven measles outbreak investigations, a similar sex-specific attack rate was reported [17, 24,25,26,27, 29, 30]. Whereas in one measles outbreak investigation, a higher sex-specific attack rate (139.4/10,000) was reported among females [28]. This might be due to the fact that women are always caregivers in some parts of Ethiopia. Therefore, there could be contact with sick children 1–4 years old.
The epidemic curve was used in all included articles to describe the outbreak in terms of time [17, 24,25,26,27,28,29,30]. Five articles were conducted from February to April [17, 26, 27, 29, 30]. This evidence was similar to the study conducted in Nigeria [32]. This might be due to high population movement and many traditional ceremonies (weddings, religious festivals) during this season or the dryness of the season, which may make the condition favorable for measles virus transmission. Two different outbreak investigations were conducted from May to July [25] and July to August [28]. In one outbreak investigation [17], the measles outbreak persisted for 117 days. A higher attack rate (91.02/10,000) was observed in subgroup analysis after 2019. This might be due to COVID-19, which causes hesitancy in outbreak investigation and response.
In seven outbreak investigations, a place-specific attack rate was used, but a map was not utilized to identify the source of the outbreak [17, 25,26,27,28,29,30]. Whereas in one measles outbreak investigation, measles cases were not described in terms of place [24]. There was a large geographical variation in the attack rate. The observed attack rates in the Amhara region were between 1.18/10,000 population and 69.9/10,000 [24, 25, 28, 29]. In three studies in the Oromia region, the observed attack rates ranged from 8.1/10,000 to 120/10,000 [17, 27, 30]. The reported attack rate in the Somalia region was 28.2/10,000 [26]. In subgroup analysis, Oromia had the highest pooled attack rate (63.05 per 10,000) [17, 27, 30], while the lowest pooled attack rate was observed in the Amhara region (17.77 per 10,000) [24, 25, 28, 29]. This discrepancy might be the difference in clusters of non-immune individuals or due to the difference in outbreak duration. In the Oromia region, the outbreak was continuing for 48 days [30], 86 days [17], and 117 days [27] whereas, in the Amhara region, the outbreak was lasting for 18 days [28], 21 days [24], 32 days [25] and 74 days [29].
The overall pooled CFR of this meta-analysis was 2.21% (95% CI: 0.07-4.36%). In two articles, the highest age-specific CFR was reported at the age of under one year, which was 3.1% [24] and 33.3% [23]. This might be due to the immaturity of the immune system.
A higher case fatality was reported after 2019, 3.35% (95% CI; 3.10-9.81%). The variation of CFR could be imposed by the difference in case management and the community’s immunity level.
Measles vaccination provides lifelong immunity [33, 34]. Low vaccination and immunization coverage lead to an increase in the incidence of measles cases [35]. Individuals who had not been vaccinated for measles were almost six times more likely to contract the measles virus than those who had been vaccinated for measles. This is supported by the study conducted in Ohio [36]. All measles cases were unvaccinated in one measles outbreak investigation [28]. In another investigation, all measles cases had an unknown vaccination status [25]. The investigation conducted in Basoliben woreda of East Gojjam Zone, Amhara Region [29], revealed that 20% of measles cases were unvaccinated. In the above investigation, 76.7% of measles cases were vaccinated. This might be due to the problems of cold chain management and vaccine administration. On the other hand, percentage of unvaccinated measles cases by other regions was: Guji zone in the Oromia region, 75% [17], Guradamole Woreda of Bale Zone, Oromia 75.5% [30], Ginnir district of Bale zone, Oromia region, 79% [27], Sekota Zuria district, Amhara, Region, 83% [24] and Somali Region, 86.2%. This non-uniform vaccination coverage might be due to problems with accessing vaccination services or vaccine hesitancy. In six measles outbreak investigations, measles vaccine effectiveness (MVE) was not computed [24,25,26,27, 29, 30]. In two investigations, the computed MVE was 82.6% [28] and 90% [31].
The measles virus is highly contagious, and 9 out of 10 susceptible people of all ages might have contracted the virus [37]. People with contact with measles cases were four times more likely to contract the measles virus than those without no contact history. This is congruent with the study conducted in Japan, Taiwan, and China [38].
Conclusion
Our findings revealed notable pooled attack and case fatality rates, with considerable divergence across different study regions. Measles infection was significantly linked to being unvaccinated and having a contact history. Strengthening routine vaccination strategies and intensifying contact tracing efforts emerge as imperative measures.
Data Availability
The data sets generated during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AOR:
-
Adjusted odd ratio
- AR:
-
Attack rate
- CFR:
-
Case fatality rate
- CI:
-
Confidence interval
- MVE:
-
Measles vaccine effectiveness
References
CDC. Outbreak investigation [Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson6/section2.html.
WHO. Measles and Rubella Surveillance and Outbreak Investigation Guidelines. 2009 [Available from: http://apps.who.int/iris/handle/10665/205481.
Ethiopian Health Nutrition Research Institute, Federal Democratic Republic of Ethiopia. Guideline on Measles surveillance and outbreak management [Internet]. Federal Democratic Republic of Ethiopia Addis Ababa; 2012.
Ismail AS, Aden MA, Abdikarim AA, Yusuf AA. Risk factors for a Measles outbreak: an unmatched case-control study in Kabridahar District, Somali Regional State, Ethiopia. Am J Epidemiol Infect Disease. 2019;7(1):1–5.
CDC. Global Measles Outbreaks. 2022 [Available from: https://www.cdc.gov/globalhealth/measles/data/global-measles-outbreaks.html.
Signs CDC. and Symptoms 2020 [Available from: https://www.cdc.gov/measles/symptoms/signs-symptoms.html.
WHO. A guide to introducing a second dose of measles vaccine into routine immunization schedules 2013 [Available from: https://www.who.int/publications/i/item/WHO-IVB-13.03.
World Health O. Measles vaccines: WHO position paper, April 2017 - recommendations. Vaccine. 2019;37(2):219–22.
Yitbarek K, Tilahun T, Debela T, Abdena D, Girma T. Measles epidemiology and vaccination coverage in Oromia Region, Ethiopia: evidence from surveillance, 2011–2018. Vaccine. 2021;39(31):4351–8.
Medić S, Petrović V, Lončarević G, Kanazir M, Begović Lazarević I, Rakić Adrović S, et al. Epidemiological, clinical, and laboratory characteristics of the Measles resurgence in the Republic of Serbia in 2014–2015. PLoS ONE. 2019;14(10):e0224009.
Biellik RJ, Davis R. The new World Health Organization recommendation on the 2-dose Measles vaccine schedule and the way forward in African Region. Pan Afr Med J. 2017;27(Suppl 3):14.
Mekonen Getahun BB, Ayesheshem Ademe B, Teshome M, Tefera et al. Epidemiology of laboratory confirmed Measles virus cases in Amhara Regional State of Ethiopia, 2004–2014. BMC Infect Dis. 2016;16(133).
Gay NJ. The theory of Measles elimination: implications for the design of elimination strategies. J Infect Dis. 2004;189(Supplement1):27–S35.
Tesfa GA, Demeke AD, Hailegebreal S, Amede ES, Ngusie HS, Kasie MN, et al. Spatial distribution and associated factors of Measles vaccination among children aged 12–23 months in Ethiopia. A spatial and multilevel analysis. Hum Vaccines Immunotherapeutics. 2022;18(1):2035558.
Daddi Jima GM, Hailemariam Z, Bekele A, Addissie A. The Ethiopian Field Epidemiology and Laboratory Traning Program: strengthening public health systems and building human resource capacity the Pan. Afr Med J. 2011;10(1):5.
Wichmann O, Hellenbrand W, Sagebiel D, Santibanez S, Ahlemeyer G, Vogt G, et al. Large Measles outbreak at a German public school, 2006. Pediatr Infect Dis J. 2007;26(9):782–6.
Belda K, Tegegne AA, Mersha AM, Bayenessagne MG, Hussein I, Bezabeh B. Measles outbreak investigation in Guji zone of Oromia Region, Ethiopia. Pan Afr Med J. 2017;27(Suppl 2).
McCormack JC, Elliffe D, Virués-Ortega J. Quantifying the effects of the differential outcomes procedure in humans: a systematic review and a meta‐analysis. J Appl Behav Anal. 2019;52(3):870–92.
Hardy RJ, Thompson SG. Detecting and describing heterogeneity in meta-analysis. Stat Med. 1998;17(8):841–56.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Petitti DB. Approaches to heterogeneity in meta-analysis. Stat Med. 2001;20(23):3625–33.
Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. 2018;74(3):785–94.
Soeken KL, Sripusanapan A. Assessing publication bias in meta-analysis. Nurs Res. 2003;52(1):57–60.
Girmay A, Dadi AF. Being unvaccinated and having a contact history increased the risk of Measles Infection during an outbreak: a finding from Measles outbreak investigation in rural district of Ethiopia. BMC Infect Dis. 2019;19(1):1–6.
Aragaw M, Tilay T. Measles outbreak in Simada District, South Gondar Zone, Region A. May-June 2009: immediate need for strengthened routine and supplemental immunization activities (SIAs). Ethiopian Journal of Health Development. 2012;26(2):115-8.
Mohammed Y, Niguse A. Measles Outbreak Investigation and Response in Jarar Zone of Ethiopian Somali Regional State, Eastern Ethiopia. Intl J. 2017;8(3):86–91.
Kalil FS, Gemeda DH, Bedaso MH, Wario SK. Measles outbreak investigation in Ginnir district of Bale Zone, Oromia region, Southeast Ethiopia, May 2019. Pan Afr Med J. 2020;36(1).
Tariku MK, Misikir SW. Measles outbreak investigation in Artuma Fursi Woreda, Oromia Zone, Amhara region, Ethiopia, 2018: a case control study. BMC Res Notes. 2019;12(1):1–6.
Tesfaye A, Sisay A, Sofoniyas G, Yimer S, Addisu M, Chalachew G. Measles outbreak investigation in Basso Liben District, Amhara Region, Ethiopia 2017. J Infect Dis Immun. 2021;13(1):1–6.
Tsegaye G, Gezahegn Y, Tesfaye A, Mulatu G, Bulcha GG, Berhanu N. Measles Outbreak Investigation in Guradamole District of Bale Zone, South Eastern Ethiopia, 2021. Infect Drug Resist. 2022;15:669.
Leuridan E, Hens N, Hutse V, Ieven M, Aerts M, Van Damme P. Early waning of maternal Measles antibodies in era of Measles elimination: longitudinal study. BMJ. 2010;340:c1626.
Fatiregun AA, Adebowale AS, Fagbamigbe AF. Epidemiology of Measles in Southwest Nigeria: an analysis of Measles case-based surveillance data from 2007 to 2012. Trans R Soc Trop Med Hyg. 2014;108(3):133–40.
Ludlow M, McQuaid S, Milner D, de Swart RL, Duprex WP. Pathological consequences of systemic Measles virus Infection. J Pathol. 2015;235(2):253–65.
Control CfD, Prevention, Program N.I., Prevention), Program N.I., Education P, et al. Epidemiology and prevention of vaccine-preventable diseases: Department of Health & Human Services, Public Health Service, Centers for …; 2005
Halsey NA, Hyman SL, Panel CW. Measles-mumps-rubella vaccine and autistic spectrum disorder: report from the New Challenges in Childhood Immunizations Conference convened in Oak Brook, Illinois, June 12–13, 2000. Pediatrics. 2001;107(5):e84-e.
Gastañaduy PA, Budd J, Fisher N, Redd SB, Fletcher J, Miller J, et al. A Measles outbreak in an underimmunized Amish community in Ohio. N Engl J Med. 2016;375(14):1343–54.
CDC. : Measles 2018 [Available from: https://www.cdc.gov/measles/contagious-infographic.html.
Shimizu K, Kinoshita R, Yoshii K, Akhmetzhanov AR, Jung S, Lee H, et al. An investigation of a Measles outbreak in Japan and China, Taiwan, China, March-May 2018. Western Pacific surveillance and response journal. WPSAR. 2018;9(3):25–31.
Acknowledgements
We would like to acknowledge all authors of investigations included in this systemic review and Meta-analysis.
Funding
This work was funded by ourselves.
Author information
Authors and Affiliations
Contributions
The primary manuscript text was authored by M.K. and S.W., while A.H. was responsible for generating Figs. 1, 2, 3, 4 and 5. D.T. undertook manuscript preparation, analysis, and PRISMA diagram creation and revision. S.A. crafted the abstract with input from all authors. Subsequently, all authors participated in the manuscript review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tariku, M.K., Worede, D.T., Belete, A.H. et al. Attack rate, case fatality rate and determinants of measles infection during a measles outbreak in Ethiopia: systematic review and meta-analysis. BMC Infect Dis 23, 756 (2023). https://doi.org/10.1186/s12879-023-08757-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08757-0