
Abstract
Background
Individuals in close contact with active pulmonary tuberculosis (TB) patients showed a high risk of recent infection and, once infected, higher risk of developing active TB in the following years post-exposure. But the peak time of active disease onset is unclear. This study aims to estimate post exposure TB incidence risk among close contacts to provide reference for clinical and public health strategies.
Methods
We searched PubMed, Web of Science, and EMBASE for articles published until December 1, 2022. The incidence rates were quantitatively summarized by means of meta-analysis using the random-effect model.
Results
Of the 5616 studies, 31 studies included in our analysis. For baseline close contacts results, the summarized prevalence of Mycobacterium tuberculosis (MTB) infection and active TB was found to be 46.30% (95% CI: 37.18%-55.41%) and 2.68% (95% CI: 2.02%-3.35%), respectively. During the follow-up, the 1-year, 2-year and 5-year cumulative incidence of TB in close contacts were 2.15% (95% CI: 1.51%-2.80%), 1.21% (95% CI: 0.93%-1.49%) and 1.11% (95% CI: 0.64%-1.58%), respectively. Individuals with a positive result of MTB infection testing at baseline showed significantly higher cumulative TB incidence as compared to those negatives (3.80% vs. 0.82%, p < 0.001).
Conclusions
Individuals with close contact to active pulmonary TB patients are bearing significant risk of developing active TB, particularly within the first-year post-exposure. Population with recent infections should be an important priority for active case finding and preventive intervention worldwide.
Similar content being viewed by others


Introduction
Globally, tens of millions of people might be exposed to Mycobacterium tuberculosis (MTB) each year [1,2,3]. According to the latest estimates by the World Health Organization (WHO),10.6 million people fell ill with TB worldwide, and 1.6 million people died from TB in 2021 [3]. Individuals in close contact with active pulmonary tuberculosis (TB) patients showed a high risk of recent infection and, once infected, a higher risk of developing active TB in the following two years post-exposure [1, 4, 5]. In many areas with a low incidence of TB, identifying and evaluating people who have come into contact with active TB patients was one important component of TB control programs [2]. WHO recommended MTB infection testing and treatment along with contact investigation for contacts of bacteriologically confirmed TB cases as well [3].
One of the purposes of conducting contact investigation is to find active cases earlier among close contacts of pulmonary TB disease, and another one is to identify the recently infected persons for further preventive treatment to protect them from developing active disease. One systematic review and meta-analysis included 41 studies reported that contact investigation was an effective tool of case finding [6]. Another meta-analysis which included 34 studies reported a summarized prevalence of active TB among household contacts was 2.3% (95% Confidence interval [CI]: 2.1%-2.5%) [7]. However, prospective studies addressing the incidence of active TB among close contacts in different periods of post-exposure were much less or long time ago [4, 5]. Therefore, the significance of expanding MTB infection testing and treatment among close contacts is not very clear in different settings with varied TB epidemics. In addition, identifying the peak time of active disease onset is also important for targeting at risk individuals for intervention more precisely. Therefore, this study aims to estimate the incidence of active TB among close contacts in different periods of post-exposure by means of systematic review and meta-analysis.
Methods
The study protocol was prospectively registered in PROSPERO (number CRD42021265151). This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards [8].
Information sources and search strategy
A systematic search of PubMed, Embase, and Web of Science was conducted from inception to December 1, 2022. Various combinations of the terms “tuberculosis”, “mycobacterium tuberculosis”, “contact tracing” and “close contact” were used to screen for potential studies reported TB incidence among contacts of active TB patients without any geographical restriction. The detailed search strategy was presented in Supplementary Files. Additional studies were also identified by cross-referencing.
Eligibility criteria
Inclusion criteria include: the study should be a prospective or retrospective cohort study and studied contacts should be followed for at least one year; the study should report original data of TB incidence among close contacts during the follow-up period. Exclusion criteria include: non-English reports if the necessary information was not reported in the abstract in English; non-original articles with repeated or incomplete data; the sample size of the studied close contacts was less than 100 [9].
Selection process
Two investigators Y Du and YJ He independently completed study screening. After duplications were removed, the two authors screened the studies in two stages: first by title and abstract and then by full text article. They independently finished study identification and data extraction, and consensus was reached on all of the items. Discrepancies were resolved by consensus with a third researcher (HR Zhang). All full texts against eligibility criteria were also checked by HR Zhang.
Data extraction
Literature management used Endnote X9.3.3. When data were reported from overlapping study samples, the most recent and comprehensive reports were considered. The extracted data include: study information (first author, publication year, study design, demographics, number of index cases, number of close contact cases, age and gender distribution, diagnosis of index case, and exposure classification of contacts), baseline investigation information (diagnosis and prevalence of TB, diagnosis and prevalence of MTB infection), and follow-up investigation information (follow-up period, diagnosis and incidence of TB).
Study definitions
Close contacts were defined as either household contacts or non-household contacts. Most of the included studies defined household contact as a person who had shared the same enclosed living space with the index case for more than one or more nights or frequent or extended daytime periods during the 3 months before the start of current treatment; most studies defined non-household as a person who was not in the household but shared an enclosed space (such as a social gathering, workplace or facility) for extended periods during the day with index case during the 3 months before the commencement of the current TB treatment episode. Most studies reported the incident TB during follow-up as confirmed cases without coprevalent disease, which was defined as confirmed TB identified at baseline or within 3 months post-exposure. Most studies took coprevalent disease into account to estimate the prevalence of active TB among close contacts at baseline. MTB infection status was defined as interferon-gamma release assay (IGRA) positive or a tuberculin skin test (TST) induration response of ≥ 10 mm in adults or ≥ 5 mm in children in most included studies. High TB burden countries were defined by WHO global TB report 2020 [3]. Only people who did not receive preventive chemotherapy were included in this analysis.
Statistical analysis
Inter-study heterogeneity was assessed by Chi-square test with significance set at the p < 0.10 level. Higgins’ I2 statistics, values range from 0 to 100%, and values ≥ 50% were considered to be indicative of substantial heterogeneity [10]. Effect size with its 95% CI was calculated with a random-effects model when heterogeneity was considerable among studies. The age of index cases was presented with mean ± standard deviation (SD) or median (Q25-Q75). Stratified analyses were conducted according to the study origin (high TB burden countries or other countries), time-period of follow-up (1-year, 2-year and 5-year), MTB infection status at baseline (positive or negative), microbiologically status of the index case (positive). Egger weighted regression method, Begg rank correlation method [11] and symmetry of the funnel plots were used to assess the possibility of publication bias with significance at the p < 0.05 [12]. All the statistical analyses were performed through STATA 12.0 (Stata Corporation, College Station, TX, USA).
Result
Study identification and characteristics of the included studies
A total of 5,616 articles were obtained by database searches using different combinations of key terms (Fig. 1). Among them, 2,653 were excluded due to overlapping and 2,552 were excluded by abstract review due to irrelevant to the study objective. Thus, 411 articles and another 12 cross-references were full text retrieved for more detailed evaluation. Of them, 46 non-original articles (i.e. abstract, letter, editorial, poster, and review) and 4 non-English articles were firstly excluded, and then 15 were excluded because the sample size of the studied contact cases was less than 100, 238 were excluded because of missing completed incidence-related data, 89 were excluded because did not perform contact tracing, finally, a total of 31 eligible articles were included in this study [4, 5, 13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] (Detailed search strategy and included studies were in Supplementary Appendix).

Identification of eligible studies on the incidence of active tuberculosis among close contacts. A total of 5,616 articles were obtained by database searches using different combinations of key terms. Among them, 2,653 records excluded because of overlap and 2,552 were excluded by abstracts review due to irrelevant to the study objective. Thus, 411 articles and another 12 cross-references were full text retrieved for more detailed evaluation. Of them, 46 non-original articles and 4 non-English articles were firstly excluded, and then 15 were excluded because the sample size of the studied contacts was less than 100, 238 were excluded because of missing completed incidence-related data, 89 were excluded because did not complete contact tracing, finally, a total of 31 eligible articles were included in this study
As shown in Table 1, publication of the included studies occurred between 1960 and 2020, and the sample size of contacts varied from 103 to 10,160. Of the 31 included studies, 21 (68%) were based on prospective design and 12 (39%) came from high TB burden countries. A total of 12,889 index cases and 53,327 contact cases were included in this analysis. For one bacteriologically confirmed pulmonary TB patient, the mean number of contacts was identified to be about 4. Most of the studied index cases were adults while their contact cases included both children and adults. Table 2 shows the included studies’ baseline results and follow-up investigation information among close contacts.
Meta-analysis of active TB incidence among close contacts
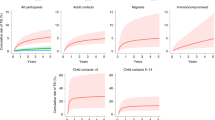
Table 3 shows the summarized active TB incidence among close contacts during the follow-up. The 1-year, 2-year and 5-year cumulative incidence rate of active TB in close contacts not receiving preventive therapy was found to be 2.15% (95% CI: 1.51%-2.80%), 1.21% (95% CI: 0.93%-1.49%) and 1.11% (95% CI: 0.64%-1.58%), respectively. Supplementary Fig. 1 showed there was no significant publication bias for 1-year cumulative incidence (Egger’s test, p = 0.448 and Begg’s test, p = 0.086), but the funnel plot seemed to be asymmetric (Supplementary Fig. 2). The 2-year active TB incidence of close contacts who exposed to TB patients with sputum smear-positives was 1.55% (95% CI: 1.08%-2.02%). Close contacts with a positive result of MTB infection testing at baseline post-exposure showed significantly higher 2-year cumulative TB incidence as compared to those negatives (3.80% vs. 0.82%, p < 0.001). Close contacts from high TB-burden countries showed higher 2-year cumulative TB incidence than those from other countries (1.63% vs. 1.03%), but the difference was not statistically significant (p = 0.057).
Meta-analysis of active TB prevalence and MTB infection prevalence among close contacts post-exposure
Of the 31 included cohort studies, 18 studies reported the baseline TB prevalence among close contacts post-exposure and the summarized estimation was 2.68% (95% CI: 2.02%-3.35%). Studies participants from high TB burden countries showed a higher baseline prevalence of TB than those from other countries (5.55% vs. 2.16%, p = 0.022) (Table 4).
In addition, 20 of the 31 included cohort studies reported the baseline MTB infection prevalence among close contacts post-exposure (Table 4), the summarized estimation was 46.30% (95% CI: 37.18%-55.41%). In 18 studies, TST was used to test MTB infection and the summarized prevalence of MTB infection was 48.37% (95% CI: 38.58%-58.16%). While 6 studies used IGRA to test MTB infection and the summarized prevalence was 41.24% (95% CI: 21.06%-61.42%). No statistically significant difference was observed between the summarized estimates based on these two tests (p = 0.571). In stratified analysis, the prevalence of MTB infection among close contacts of sputum smear-positive index cases was 53.94% (95% CI: 41.76%-66.12%). No statistically significant difference in summarized MTB infection prevalence among the close contacts was observed between studies from high TB burden countries and other countries included in the review(52.80% vs. 43.51%, p = 0.433).
Discussion
The present study systematically reviewed the published cohort studies addressing the risk of active TB development among close contacts post-exposure. We found the cumulative incidence of active TB among close contacts was very high especially within the first-year post-exposure. The stratified analyses showed that contacts exposed to microbiologically confirmed pulmonary TB patients should be given priority for active TB screening and MTB infection testing and treatment, especially in the areas with high TB burden.
According to the WHO’s recommendations for middle- and low-income countries [42, 43], besides children younger than 5 years and people living with HIV, other risk populations such as close contacts of TB patients should also be screened to find active TB. It has been a national strategy in China to conduct active TB case tracing and provide free screening tests to close contacts of smear-positive TB patients since 2006 (Bureau of disease prevention and control under the ministry of health, 2006) [44]. This work has been systematically evaluated to some extent, but the national data was still scarce. Therefore, it is urgently needed to develop national guidelines providing precise intervention tools and standards for protecting close contacts from MTB infection and active disease development. After exposure, close contacts might present varied outcomes depending on their immune status and degree of exposure (exposure duration, disease severity of the index cases, etc.), including infection, infection clearance, and post-infection morbidity [45]. Therefore, under the influence of many factors, it is a challenge to carry out precise interventions based on an individual’s risk. Our meta-analysis results supported the findings of several individual reports that the first-year post-exposure was the peak period of developing the active disease for close contacts, which is similar to the findings of 2-year post-exposure was estimated as a high-risk period [4, 5, 17, 25, 30, 46]. The results of the meta-analysis are very helpful to define the screening priority more precisely, especially in developing or underdeveloped countries with limited resources.
We found few studies reported TB incidence among close contacts whose index case was smear negative. Haldar P [26] found that the 2-year TB incidence among close contacts was 2.6% for those exposed to sputum smear-positive index cases and only 0.7% for those exposed to sputum smear-negative index cases. On the contrary, Triasih R [23] and Guo J [47] found that TB incidence density among close contacts was not significantly different concerning the microbiological status of the index cases. In this review, there was no significant difference in active TB incidence across the baseline characteristics of close contact with microbiologically confirmed patients. Varied study populations and different TB epidemics in the study area might contribute to the heterogeneity observed between the different studies. However, based on the results of our review of MTB infection prevalence in post-exposure close contact populations, there are still reasons to believe that investigations among close contacts of people with bacteriologically confirmed pulmonary TB should be intensified. It should be a cost-effective option both for the early TB case finding and for implement of preventive treatment among close contacts.
TB is now understood as a dynamic multistate gradient from infection acquisition to subclinical disease and clinically active disease. The outcome of exposure to active TB patients was determined by a complex interaction of bacterial, host, and environmental factors [48]. For the host, the initial exposure gradient, such as bacterial load, disease severity of the index case, and the closeness and duration of the contact, were directly associated with the risk of developing primary disease [49]. In addition, the endogenous recurrence of TB was found to be mainly associated with weakened immunity of the host [50]. Individuals with a positive result of MTB infection testing post-exposure were found under significantly higher risk of active TB incidence as compared to those negatives. Similarly, in one meta-analysis included 46 cohort studies on exposed children [9], children with a positive result for MTB infection had significantly higher 2-year cumulative TB incidence than those negatives. MTB infection testing was essential for determining the priority individuals for MTB infection screening and preventive therapy in most populations except for immunocompromised ones such as HIV infections. Because the currently available MTB infection testing, TST and IGRA, were both immunological methods with limited sensitivity in the application of immune deficiency populations. Therefore, WHO recommended TB preventive treatment for HIV infections and children aged < 5 years who are household contacts even if MTB infection testing is unavailable [51]. However, MTB infection testing should be a priority action for the general population with close contact, it has been suggested to be a good practice to identify recent conversions before initiating TB preventive treatment [52].
Limitations
There are several limitations in this review. First, the pooled analysis of all studies showed substantial heterogeneity across studies. Second, the literature describing the results of contact investigations were not easy to be systematically summarized. The quality of some literature was poor and the critical information for estimating incidence might frequently be missed. Such studies might be excluded which made our study results generalization limited. Also, some retrospective studies were included in this review, they could be attributed to, at least partially, to the presence of confounders, which then lower the power of generalization of the findings. Third, missing essential data also limited more detailed stratified analyses, such as many studies only reported 2-year TB incidence post-exposure, but 1-year estimate were less reported. These three databases cannot cover all related studies, and non-English reports were excluded if the necessary information was not reported in the abstract in English, such eligibility criteria might cause selection bias.
Conclusion
Our review suggested that close contacts of patients with microbiologically confirmed pulmonary TB are a group at high risk of developing active TB, particularly within the first-year post-exposure. It may imply that expanding close contacts investigation in more at-risk populations is of great significance both for the early detection of TB and for precisely identifying MTB infection treatment targets. In addition, we should continuously optimize the guidelines to improve the quality of close contacts management combined with local public health resources and the TB epidemic situation.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- TB:
-
Tuberculosis
- MTB:
-
Mycobacterium tuberculosis
- WHO:
-
World Health Organization
- CI:
-
Confidence interval
- IGRA:
-
Interferon gamma release assay
- TST:
-
Tuberculin skin test
References
Grzybowski S, Barnett GD, Styblo K. Contacts of cases of active pulmonary tuberculosis. Bull Int Union Tuberc. 1975;50(1):90–106.
Taylor Z, Nolan CM, Blumberg HM. Controlling tuberculosis in the United States. Recommendations from the American Thoracic Society, CDC, and the Infectious Diseases Society of America. MMWR Recomm Rep. 2005;54(Rr-12):1–81.
World Health Organization. Global Tuberculosis Report 2022. 2022. Available from: https://www.who.int/publications/i/item/9789240061729. Accessed 1 Feb 2023
Yassin MA, Yirdaw KD, Datiko DG, Cuevas LE, Yassin MA. Yield of household contact investigation of patients with pulmonary tuberculosis in southern Ethiopia. BMC Public Health. 2020;20(1):737. https://doi.org/10.1186/s12889-020-08879-z.
Saunders MJ, Tovar MA, Collier D, Baldwin MR, Montoya R, Valencia TR, et al. Active and passive case-finding in tuberculosis-affected households in Peru: a 10-year prospective cohort study. Lancet Infect Dis. 2019;19(5):519–28. https://doi.org/10.1016/s1473-3099(18)30753-9.
Morrison J, Pai M, Hopewell PC. Tuberculosis and latent tuberculosis infection in close contacts of people with pulmonary tuberculosis in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2008;8(6):359–68. https://doi.org/10.1016/s1473-3099(08)70071-9.
Fox GJ, Barry SE, Britton WJ, Marks GB. Contact investigation for tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2013;41(1):140–56. https://doi.org/10.1183/09031936.00070812.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Martinez L, Cords O, Horsburgh CR, Andrews JR. The risk of tuberculosis in children after close exposure: a systematic review and individual-participant meta-analysis. Lancet. 2020;395(10228):973–84. https://doi.org/10.1016/s0140-6736(20)30166-5.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ (Clinical research ed). 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ (Clinical research ed). 1997;315(7109):629–34. https://doi.org/10.1136/bmj.315.7109.629.
Araújo NCN, Cruz CMS, Arriaga MB, Cubillos-Angulo JM, Rocha MS, Silveira-Mattos PS, et al. Determinants of losses in the latent tuberculosis cascade of care in Brazil: A retrospective cohort study. Int J Infect Dis. 2020;93:277–83. https://doi.org/10.1016/j.ijid.2020.02.015.
Huerga H, Sanchez-Padilla E, Melikyan N, Atshemyan H, Hayrapetyan A, Ulumyan A, et al. High prevalence of infection and low incidence of disease in child contacts of patients with drug-resistant tuberculosis: a prospective cohort study. Arch Dis Child. 2019;104(7):622–8. https://doi.org/10.1136/archdischild-2018-315411.
Benjumea-Bedoya D, Marín DM, Robledo J, Barrera LF, López L, Del Corral H, et al. Risk of infection and disease progression in children exposed to tuberculosis at home Colombia. Colomb Med (Cali). 2019;50(4):261–74. https://doi.org/10.25100/cm.v50i4.4185.
Becerra MC, Huang CC, Lecca L, Bayona J, Contreras C, Calderon R, et al. Transmissibility and potential for disease progression of drug resistant Mycobacterium tuberculosis: prospective cohort study. BMJ (Clinical research ed). 2019;367:l5894. https://doi.org/10.1136/bmj.l5894.
Reichler MR, Khan A, Sterling TR, Zhao H, Moran J, McAuley J, et al. Risk and Timing of Tuberculosis Among Close Contacts of Persons with Infectious Tuberculosis. J Infect Dis. 2018;218(6):1000–8. https://doi.org/10.1093/infdis/jiy265.
Martinez L, Shen Y, Handel A, Chakraburty S, Stein CM, Malone LL, et al. Effectiveness of WHO’s pragmatic screening algorithm for child contacts of tuberculosis cases in resource-constrained settings: a prospective cohort study in Uganda. Lancet Respir Med. 2018;6(4):276–86. https://doi.org/10.1016/s2213-2600(17)30497-6.
Baliashvili D, Kempker RR, Blumberg HM, Kuchukhidze G, Merabishvili T, Aslanikashvili A, et al. A population-based tuberculosis contact investigation in the country of Georgia. Public Health Action. 2018;8(3):110–7. https://doi.org/10.5588/pha.18.0024.
Sharma SK, Vashishtha R, Chauhan LS, Sreenivas V, Seth D. Comparison of TST and IGRA in Diagnosis of Latent Tuberculosis Infection in a High TB-Burden Setting. PLoS ONE. 2017;12(1):e0169539. https://doi.org/10.1371/journal.pone.0169539.
Puma DV, Pérez-Quílez O, Roure S, Martínez-Cuevas O, Bocanegra C, Feijoo-Cid M, et al. Risk of Active Tuberculosis among Index Case of Householders-A Long-Term Assessment after the Conventional Contacts Study. Public Health Nurs. 2017;34(2):112–7. https://doi.org/10.1111/phn.12279.
Muñoz L, Gonzalez L, Soldevila L, Dorca J, Alcaide F, Santin M. QuantiFERON®-TB Gold In-Tube for contact screening in BCG-vaccinated adults: A longitudinal cohort study. PLoS ONE. 2017;12(8):e0183258. https://doi.org/10.1371/journal.pone.0183258.
Triasih R, Robertson C, Duke T, Graham SM. Risk of infection and disease with Mycobacterium tuberculosis among children identified through prospective community-based contact screening in Indonesia. Trop Med Int Health. 2015;20(6):737–43. https://doi.org/10.1111/tmi.12484.
Chakhaia T, Magee MJ, Kempker RR, Gegia M, Goginashvili L, Nanava U, et al. High utility of contact investigation for latent and active tuberculosis case detection among the contacts: a retrospective cohort study in Tbilisi, Georgia, 2010–2011. PLoS ONE. 2014;9(11):e111773. https://doi.org/10.1371/journal.pone.0111773.
Singh J, Sankar MM, Kumar S, Gopinath K, Singh N, Mani K, et al. Incidence and prevalence of tuberculosis among household contacts of pulmonary tuberculosis patients in a peri-urban population of South Delhi, India. PLoS ONE. 2013;8(7):e69730. https://doi.org/10.1371/journal.pone.0069730.
Haldar P, Thuraisingam H, Patel H, Pereira N, Free RC, Entwisle J, et al. Single-step QuantiFERON screening of adult contacts: a prospective cohort study of tuberculosis risk. Thorax. 2013;68(3):240–6. https://doi.org/10.1136/thoraxjnl-2011-200956.
Wang JY, Shu CC, Lee CH, Yu CJ, Lee LN, Yang PC. Interferon-gamma release assay and Rifampicin therapy for household contacts of tuberculosis. J Infect. 2012;64(3):291–8. https://doi.org/10.1016/j.jinf.2011.11.028.
Song S, Jeon D, Kim JW, Kim YD, Kim SP, Cho JS, et al. Performance of confirmatory interferon-γ release assays in school TB outbreaks. Chest. 2012;141(4):983–8. https://doi.org/10.1378/chest.11-1158.
Denholm JT, Leslie DE, Jenkin GA, Darby J, Johnson PD, Graham SM, et al. Long-term follow-up of contacts exposed to multidrug-resistant tuberculosis in Victoria, Australia, 1995–2010. Int J Tuberc Lung Dis. 2012;16(10):1320–5. https://doi.org/10.5588/ijtld.12.0092.
Becerra MC, Appleton SC, Franke MF, Chalco K, Arteaga F, Bayona J, et al. Tuberculosis burden in households of patients with multidrug-resistant and extensively drug-resistant tuberculosis: a retrospective cohort study. Lancet. 2011;377(9760):147–52. https://doi.org/10.1016/s0140-6736(10)61972-1.
Lienhardt C, Fielding K, Hane AA, Niang A, Ndao CT, Karam F, et al. Evaluation of the prognostic value of IFN-gamma release assay and tuberculin skin test in household contacts of infectious tuberculosis cases in Senegal. PLoS ONE. 2010;5(5):e10508. https://doi.org/10.1371/journal.pone.0010508.
del Corral H, París SC, Marín ND, Marín DM, López L, Henao HM, et al. IFNgamma response to Mycobacterium tuberculosis, risk of infection and disease in household contacts of tuberculosis patients in Colombia. PLoS ONE. 2009;4(12):e8257. https://doi.org/10.1371/journal.pone.0008257.
Cailleaux-Cezar M, de A Melo D, Xavier GM, de Salles CL, de Mello FC, Ruffino-Netto A, et al. Tuberculosis incidence among contacts of active pulmonary tuberculosis. Int J Tuberc Lung Dis. 2009;13(2):190–5. https://doi.org/10.1371/journal.pone.0001379.
Hill PC, Jackson-Sillah DJ, Fox A, Brookes RH, de Jong BC, Lugos MD, et al. Incidence of tuberculosis and the predictive value of ELISPOT and Mantoux tests in Gambian case contacts. PLoS ONE. 2008;3(1):e1379. https://doi.org/10.1371/journal.pone.0001379.
Diel R, Loddenkemper R, Meywald-Walter K, Niemann S, Nienhaus A. Predictive value of a whole blood IFN-gamma assay for the development of active tuberculosis disease after recent infection with Mycobacterium tuberculosis. Am J Respir Crit Care Med. 2008;177(10):1164–70. https://doi.org/10.1164/rccm.200711-1613OC.
Lemos AC, Matos ED, Pedral-Sampaio DB, Netto EM. Risk of tuberculosis among household contacts in Salvador. Bahia Braz J Infect Dis. 2004;8(6):424–30. https://doi.org/10.1590/s1413-86702004000600006.
Bayona J, Chavez-Pachas AM, Palacios E, Llaro K, Sapag R, Becerra MC. Contact investigations as a means of detection and timely treatment of persons with infectious multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2003;7(12 Suppl 3):S501–9.
Devadatta S, Dawson JJ, Fox W, Janardhanam B, Radhakrishna S, Ramakrishnan CV, et al. Attack rate of tuberculosis in a 5-year period among close family contacts of tuberculous patients under domiciliary treatment with isoniazid plus PAS or isoniazid alone. Bull World Health Organ. 1970;42(3):337–51.
Kamat SR, Dawson JJ, Devadatta S, Fox W, Janardhanam B, Radhakrishna S, et al. A controlled study of the influence of segregation of tuberculous patients for one year on the attack rate of tuberculosis in a 5-year period in close family contacts in South India. Bull World Health Organ. 1966;34(4):517–32.
Ramakrishnan CV, Andrews RH, Devadatta S, Fox W, Radhakrishna S, Somasundaram PR, et al. Influence of segregation to tuberculous patients for one year on the attack rate of tuberculosis in a 2-year period in close family contacts in South India. Bull World Health Organ. 1961;24(2):129–48.
Andrews RH, Devadatta S, Fox W, Radhakrishna S, Ramakrishnan CV, Velu S. Prevalence of tuberculosis among close family contacts of tuberculous patients in South India, and influence of segregation of the patient on early attack rate. Bull World Health Organ. 1960;23(4–5):463–510.
WHO Guidelines Approved by the Guidelines Review Committee. Recommendations for Investigating Contacts of Persons with Infectious Tuberculosis in Low- and Middle-Income Countries. Geneva: World Health Organization Copyright © World Health Organization; 2012.
Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO’s new end TB strategy. Lancet. 2015;385(9979):1799–801. https://doi.org/10.1016/s0140-6736(15)60570-0.
Bureau of Disease Prevention and Control under the Ministry of Health. Guidelines for contact investigation of sputum smear positive tuberculosis (in Chinese). 2006;224.
Pai M, Behr MA, Dowdy D, Dheda K, Divangahi M, Boehme CC, et al. Tuberculosis. Nat Rev Dis Primers. 2016;2:16076. https://doi.org/10.1038/nrdp.2016.76.
Saunders MJ, Wingfield T, Tovar MA, Baldwin MR, Datta S, Zevallos K, et al. A score to predict and stratify risk of tuberculosis in adult contacts of tuberculosis index cases: a prospective derivation and external validation cohort study. Lancet Infect Dis. 2017;17(11):1190–9. https://doi.org/10.1016/s1473-3099(17)30447-4.
Guo J, Yang M, Wu Z, Shen X, Wang Y, Zhao G. High incidence and low case detection rate among contacts of tuberculosis cases in Shanghai, China. BMC Infect Dis. 2019;19(1):320. https://doi.org/10.1186/s12879-019-3942-2.
Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection. N Engl J Med. 2015;372(22):2127–35. https://doi.org/10.1056/NEJMra1405427.
Saunders MJ, Wingfield T, Datta S, Montoya R, Ramos E, Baldwin MR, et al. A household-level score to predict the risk of tuberculosis among contacts of patients with tuberculosis: a derivation and external validation prospective cohort study. Lancet Infect Dis. 2020;20(1):110–22. https://doi.org/10.1016/s1473-3099(19)30423-2.
Selwyn PA, Hartel D, Lewis VA, Schoenbaum EE, Vermund SH, Klein RS, et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med. 1989;320(9):545–50. https://doi.org/10.1056/nejm198903023200901.
World Health Organization. The End TB Strategy. 2015. Available from: https://www.who.int/teams/global-tuberculosis-programme/the-end-tb-strategy. Accessed 29 Apr 2021.
Horsburgh CR Jr. Priorities for the treatment of latent tuberculosis infection in the United States. N Engl J Med. 2004;350(20):2060–7. https://doi.org/10.1056/NEJMsa031667.
Acknowledgements
We appreciate the assistance of YJ Li (a reference librarian, Capital Medical University, Beijing, China) for her help with validation of search strategy.
Funding
This work was supported by the National Science and Technology Major Project of China [2017ZX10201302-002 and 2017ZX10201302-009]; and the CAMS Innovation Fund for Medical Sciences (CIFMS) [2019-I2M-2–005 and 2021–1-I2M-2–037].
Author information
Authors and Affiliations
Contributions
Y D, YJ H, and HR Z had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis; L Gao, JM L, F S, L Guan, HN X, YP H, XF C, BX F and ZS Q conceived and designed the study; Y D, YJ H and HR Z performed the statistical analysis; Y D and L Gao wrote the report. All authors critically revised the manuscript for important intellectual content and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Du, Y., He, Y., Zhang, H. et al. Declining incidence rate of tuberculosis among close contacts in five years post-exposure: a systematic review and meta-analysis. BMC Infect Dis 23, 373 (2023). https://doi.org/10.1186/s12879-023-08348-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08348-z