
Abstract
Aim
Until now, the performance of interferon-γ release assay (IGRA) and Mantoux tests remains unclear in infant tuberculous meningitis (TBM). Therefore, a systematic review is performed to evaluate the sensitivity of IGRA and Mantoux tests for the diagnosis of infant TBM in low and intermediate tuberculosis (TB) burden countries, while following PRISMA.
Methods
Several databases, including PubMed, EBSCO, Embase, Scopus, Web of Science, ClinicalTrials.gov, and Cochrane Central Register of Controlled Trials, were searched. Articles describing the results of IGRA or Mantoux tests among infant TBM were included for analysis. Data, such as age, sex, Mantoux test or IGRA, and cerebrospinal fluid (CSF) microbiological examinations (such as acid-fast bacilli (AFB) smear, TB PCR, and TB culture), were extracted from each study.
Results
A total of 31 articles were enrolled for further analysis, including 48 cases. The mean age was 9.4 ± 5.8 months and boys accounted for 57.1% of infants (24/42). Mantoux test was positive in 57.4% (27/47) of tested infants and IGRA was positive in 77.8% (7/9) of infants. In addition, among the infants with confirmed TB, 18 (52.9%, 18/34) of them have positive Mantoux responses and 7 (20.0%, 7/35) have positive IGRA results.
Conclusions
In low or intermediate TB burden countries, the Mantoux test has a poor performance for diagnosing TBM among infants, and IGRAs appear to have a moderate sensitivity for the diagnosis of infant TBM.
Similar content being viewed by others


Background
Currently, tuberculosis (TB) remains a major threat to child health. According to the WHO Global Tuberculosis Report (2021), 9.9 million people were estimated to fall ill with TB and children accounted for 11% of them [1]. As a severe form of TB, tuberculous meningitis (TBM) accounted for approximately 10% of all TB children [2]. Moreover, a meta-analysis revealed a death rate of 19.3% in TBM children [3]. Fortunately, accumulated evidence is made in terms of the management of childhood TBM, and a declined TBM incidence was observed in a cross-sectional study from 2006 to 2011 [4]. However, the diagnosis of childhood TBM is often a challenge because of the nonspecific clinical presentation and the lack of a sufficiently sensitive microbiological tool for the diagnosis. Therefore, further investigation is required to improve the strategy of diagnosis for this disease,
Young age is considered a potent risk factor for TBM, while Bacillus Calmette-Guérin (BCG) vaccination is protective, particularly in young children [5]. Infant TBM is rarely reported. However, In China, TBM accounted for 19.1% of all TB infants [6]. Currently, almost all studies of infant TBM are case reports and no reliable evidence is provided to improve its management, and most treatment choices are copied from the experience of childhood TBM directly. Hence, an effort is needed to review the characteristics of infant TBM and improve its current dilemma.
In general, the diagnostic value of interferon-γ release assay (IGRA) or Mantoux response is limited in high TB burden countries, and usually no intervention is given when there is a positive result. However, in low and intermediate TB burden countries, if positive results for interferon-γ release assay (IGRA) or Mantoux response were observed, isoniazid preventive therapy may be then initiated after active TB is ruled out, and the value of positive results were therefore significant. Besides, these tests could facilitate the diagnosis of TBM [7]. Unfortunately, false-negative results of IGRA remain a concern among childhood TB, and approximately 15% of culture-confirmed TB children were IGRA-negative [8], and children with an age of < 2 years were more likely to have a negative IGRA response [9]. Therefore, the actual performance of IGRA and Mantoux tests require to be investigated, especially in infant TB. In this study, a systematic review is performed aiming to evaluate the sensitivity of IGRA and Mantoux tests for diagnosing infant TBM.
Methods
Literature searching
On October 14th, 2021, several databases, including PubMed, EBSCO, Embase, Scopus, Web of Science, ClinicalTrials.gov, and Cochrane Central Register of Controlled Trials, were searched, while following PRISMA guidelines. The full search strategies are described in Supplementary materials. Two authors independently screened the reports, and a third arbitrated disagreements between them (HJ, HY, and WMS).
Eligibility criteria
Articles describing the results of IGRA or Mantoux tests among infant TBM were eligible for inclusion. Infants were defined as ≤ 24 months. There is no requirement of study design or language. Duplicates were automatically detected by a reference manager and reduced to a single one. Other exclusion criteria included: published before 2000, unavailable full text, Non-TBM, no IGRA or Mantoux data, and duplicates. Data extracted from each study included the following items: first author, country, age, sex, Mantoux test or IGRA, cerebrospinal fluid (CSF) microbiological examinations (such as acid-fast bacilli (AFB) smear, TB PCR, and TB culture), Mycobacterium tuberculosis, Bacille Calmette-Guérin (BCG) vaccination. A diagnosis of confirmed TB (or TBM) was made if non-central nervous system (non-CNS, or CNS) samples were AFB smear-, TB-PCR- or culture-positive.
Statistical analysis
Data were analyzed using SPSS 16.0. Continuous variables were reported as median ± interquartile range (IQR) and categorical variables were reported as frequencies (percentages). Continuous variables were also transformed into categorical variables for further analysis if applicable. In addition, the association between Mantoux results and age or sex was analyzed using univariate logistic regression analysis.
Results
Literature selection
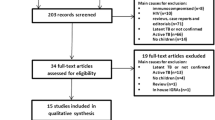
A total of 11,452 records were identified, and then duplicates (n = 7849) were removed. The remaining records (n = 3063) were screened and excluded based on title and abstract, and only 128 articles were left for qualitative review. Subsequently, 99 articles were excluded due to: unavailable full text (n = 10); age (> 24 months; n = 11); duplicates (n = 1); non-TBM (n = 8); incomplete data (n = 5), no TST or IGRA results (n = 40), and high TB burden countries (n = 22). Finally, 31 articles were enrolled for further analysis, including 48 cases (Fig. 1).

Literature selection
Baseline characteristics
The mean age was 9.4 ± 5.8 months and boys accounted for 57.1% of infants (24/42). Mantoux test was positive in 57.4% (27/47) of tested infants and IGRA was positive in 77.8% (7/9) of infants. Of the 47 cases, twenty-six were confirmed with CSF findings, including AFB smear (+, n = 4), PCR (+, n = 13), and culture (+, n = 18). Non-CNS TB evidence were found in 27 patients, including AFB (+, n = 10), PCR (+, n = 9), and culture (+, n = 20). Based on non-CSF and CSF findings, a total of 35 cases were found with microbiological evidence. The details are listed in Supplementary Table 1.
Mantoux and IGRA results
The Mantoux and IGRA results are listed in Table 1. Of the infants with confirmed TBM (n = 26), 25 (96.2%, 25/26) were tested with Mantoux test and 14 (56.0%, 14/25) of them were positive, 6 (23.1%, 6/26) were tested with IGRAs and 4 (66.7%, 4/6) of them were positive. Of the infants with confirmed TB elsewhere (non-CNS, n = 27), 27 (100%, 27/27) were tested with Mantoux test and 17 (63.0%, 17/27) of them were positive, 5 (18.5%, 5/27) were tested with IGRAs and 4 (80.0%, 4/5) of them were positive. In addition, among the infants with confirmed TB (n = 35), 34 (97.1%, 34/35) were tested with Mantoux test and 18 (52.9%, 18/34) of them were positive, 7 (20.0%, 7/35) were tested with IGRAs and 5 (71.4%, 5/7) of them were positive. IGRAs and Mantoux test were performed in 9 infants, discordance between IGRAs and Mantoux results was found in three cases (including an indeterminate response, n = 1).
In addition, among infants with BCG vaccination (n = 15), 8 (53.3%) of them were Mantoux-positive. An interesting finding was also observed, this is that three TBM infants have conversion results of Mantoux test (before anti-TB therapy, n = 1; during anti-TB therapy, n = 2). Further analysis was performed to evaluate the association between age (or sex) and Mantoux responses. However, no significant correlation was found (age, P = 0.405; sex, P = 0.829).
Discussion
Infants are considered at high risk of TBM. First, infants have a higher likelihood of progression from infection to active TB and even dissemination occurs, leading to severe TB disease (such as TBM) [10]. Second, infants have underdeveloped cell-mediated immunity, which could lead to a rapid progress of the disease before the initiation of treatment. Third, due to the anatomical underdevelopment of cranial arteries and narrow cerebrospinal passages, cerebral infarction and hydrocephalus occur easily, following meningeal changes caused by immunological response against TB. Unfortunately, the tools for diagnosis of infant TBM are imperfect and incompletely characterized, this disadvantage makes the management more difficult.
As known, most studies of TBM infants were described as case reports. To our knowledge, the study is the first report to investigate the diagnostic yield of IGRA or Mantoux test for infant TBM. This systematic review demonstrated that in low and intermediate burden countries, TBM infants have a relatively low positive rate of Mantoux test and a relatively high positivity of IGRA. Similarly, a low positive rate of Mantoux response was observed in TBM infants with BCG vaccination. Therefore, caution is required to understand the value of Mantoux responses among these countries. As known, a false-negative Mantoux response would lower the suspicion of TB disease significantly.
In the study, among the infants with confirmed TB, approximately half of them have a positive Mantoux response. Moreover, previous BCG immunization had no significant effect on the reaction to tuberculin and repeat Mantoux test may increase its positive rate. In a meta-analysis, it was demonstrated that Mantoux test has a comparable sensitivity with IGRAs (ELISA, 70%; ELISPOT, 62%) for the diagnosis of childhood TB [11], the poor performance of Mantoux test remains a significant concern for childhood TB, especially in infants. Duque-Silva A, et al. described the epidemiology of pediatric CNS TB in USA, and found that Mantoux test results were negative in 38.2% of 170 CNS TB cases tested [12]. Furthermore, Mantoux test was significantly more likely to be negative in children with younger age [13]. In Papua New Guinea, Murtagh K found that among confirmed children under 2 years, 25 (71%) showed no Mantoux reaction [14]. Besides, in children with younger age, the discordance between TST and IGRA are more common than the other age group [15]. We believe that the Mantoux test has limited contribution for infant TBM diagnosis in low TB burden counties. However, based on our findings, a repeat Mantoux test is highly recommended, this would facilitate the diagnosis of infant TB. Because, this point has not been recommended for the diagnosis of infant TB.
IGRAs showed a good performance for infant TBM diagnosis, with a positive rate of 77.8%. The usefulness of IGRA in infant TB has been proved previously. For example, QuantiFERON-TB Gold In-Tube test was evaluated in 19 French immunocompetent children with active TB, and the rates of positivity were 6/10 and 9/9 in < 2 and 2- to 5-year-old children, respectively [16]. Similar findings were observed in another study: Compared with culture, the sensitivity of QuantiFERON-TB-Gold in-tube assay was 93.9%, 100%, and 94.4% in TB children ≤ 2, 2 to 5, and 5 to 16 years of age, respectively [17]. However, according to the guidelines published by the CDC, caution is warranted when using IGRAs in children aged < 5 years [18]. This is because few performance data exist for IGRA in children with younger age. Although IGRAs appear to be a good diagnostic tool for infant TBM, several cautions should be paid, when using the IGRA for infant TBM diagnosis. First, the false-negative result in confirmed childhood TB remains a concern [8]; second, TBM is known as a risk factor for false-negative IGRA results [19, 20]; third, children with younger age were significantly associated with indeterminate or negative IGRA results [21, 22].
Although our study provides valuable insights concerning infant TBM, several limitations must be recognized. First, this study has a retrospective nature, a selection bias is unavailable. Second, the sample size is small, data must be updated if new studies are published, especially IGRAs results. Third, due to the data must be collected from previous reports, the data-missing problem should be acknowledged, such as the measurement value of Mantoux response. Fourth, in our study, a 5 mm cut-off value was used for Mantoux response. Hence, the positive rate of Mantoux test is over-determined, especially in infants with BCG vaccination [23]. Additionally, since only TBM patients were included, the specificity has not been evaluated.
Conclusions
In low or intermediate TB burden countries, the Mantoux test has a poor performance for diagnosing TBM among infants. However, a repeat Mantoux test may improve its performance. Moreover, IGRAs appear to be an accurate tool for infant TBM diagnosis, although further evidence is required to validate it.
Data availability
The data used to support the findings of this study are included within the supplementary information file(s).
References
WHO. Global tuberculosis report 2021. Geneva: World Health Organization; 2021.
Wang MS, Wang JL, Liu XJ. Epidemiological Trends in the form of Childhood Tuberculosis in a Referral Tuberculosis Hospital in Shandong, China. Biomed Res Int. 2020;2020:6142567. https://doi.org/10.1155/2020/6142567.
Chiang SS, Khan FA, Milstein MB, Tolman AW, Benedetti A, Starke JR, et al. Treatment outcomes of childhood tuberculous meningitis: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14(10):947–57. https://doi.org/10.1016/s1473-3099(14)70852-7.
Chaya S, Dangor Z, Solomon F, Nzenze SA, Izu A, Madhi SA. Incidence of tuberculosis meningitis in a high HIV prevalence setting: time-series analysis from 2006 to 2011. Int J Tuberc Lung Dis. 2016;20(11):1457–62. https://doi.org/10.5588/ijtld.15.0845.
Seddon JA, Tugume L, Solomons R, Prasad K, Bahr NC, Tuberculous Meningitis International Research C. The current global situation for tuberculous meningitis: epidemiology, diagnostics, treatment and outcomes. Wellcome Open Res. 2019;4:167. https://doi.org/10.12688/wellcomeopenres.15535.1.
Li RL, Wang JL, Wang XF, Wang MS. Tuberculosis in infants: a retrospective study in China. Springerplus. 2016;5:546. https://doi.org/10.1186/s40064-016-2184-7.
Marais S, Thwaites G, Schoeman JF, Torok ME, Misra UK, Prasad K, et al. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. 2010;10(11):803–12. https://doi.org/10.1016/S1473-3099(10)70138-9.
Wang MS, Liu XJ. Risk factors for false-negative Interferon-gamma release assay results in culture-confirmed childhood TB. Am J Trop Med Hyg. 2019;101(6):1303–7. https://doi.org/10.4269/ajtmh.18-0684.
Basu Roy R, Sotgiu G, Altet-Gomez N, Tsolia M, Ruga E, Velizarova S, et al. Identifying predictors of interferon-gamma release assay results in pediatric latent tuberculosis: a protective role of bacillus Calmette-Guerin?: a pTB-NET collaborative study. Am J Respir Crit Care Med. 2012;186(4):378–84. https://doi.org/10.1164/rccm.201201-0026OC.
Bang ND, Caws M, Truc TT, Duong TN, Dung NH, Ha DTM, et al. Clinical presentations, diagnosis, mortality and prognostic markers of tuberculous meningitis in vietnamese children: a prospective descriptive study. BMC Infect Dis. 2016;16(1):573. https://doi.org/10.1186/s12879-016-1923-2.
Sun L, Xiao J, Miao Q, Feng WX, Wu XR, Yin QQ, et al. Interferon gamma release assay in diagnosis of pediatric tuberculosis: a meta-analysis. FEMS Immunol Med Microbiol. 2011;63(2):165–73. https://doi.org/10.1111/j.1574-695X.2011.00838.x.
Duque-Silva A, Robsky K, Flood J, Barry PM. Risk factors for Central Nervous System Tuberculosis. Pediatrics. 2015;136(5):e1276–84. https://doi.org/10.1542/peds.2014-3958.
Kimerling ME, Vaughn ES, Dunlap NE. Childhood tuberculosis in Alabama: epidemiology of disease and indicators of program effectiveness, 1983 to 1993. Pediatr Infect Dis J. 1995;14(8):678–84.
Murtagh K. Unreliability of the Mantoux test using 1 TU PPD in excluding childhood tuberculosis in Papua New Guinea. Arch Dis Child. 1980;55(10):795–9. https://doi.org/10.1136/adc.55.10.795.
Shah I, Kathwate J, Shetty NS. Comparison of tuberculin skin test and QuantiFERON-TB gold In-Tube test in Bacillus Calmette-Guerin-vaccinated children. Lung India. 2020;37(1):24–9. https://doi.org/10.4103/lungindia.lungindia_304_19.
Debord C, De Lauzanne A, Gourgouillon N, Guerin-El Khourouj V, Pedron B, Gaudelus J, et al. Interferon-gamma release assay performance for diagnosing tuberculosis disease in 0- to 5-year-old children. Pediatr Infect Dis J. 2011;30(11):995–7. https://doi.org/10.1097/INF.0b013e3182272227.
Lombardi G, Pellegrino MT, Denicolo A, Corsini I, Tadolini M, Bergamini BM, et al. QuantiFERON-TB performs better in children, including infants, than in adults with active tuberculosis: a Multicenter Study. J Clin Microbiol. 2019;57(10). https://doi.org/10.1128/JCM.01048-19.
Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, et al. Updated guidelines for using Interferon Gamma release assays to detect Mycobacterium tuberculosis infection - United States, 2010. MMWR Recomm Rep. 2010;59(RR–5):1–25.
Lee YM, Park KH, Kim SM, Park SJ, Lee SO, Choi SH, et al. Risk factors for false-negative results of T-SPOT.TB and tuberculin skin test in extrapulmonary tuberculosis. Infection. 2013;41(6):1089–95. https://doi.org/10.1007/s15010-013-0478-z.
Di L, Li Y. The risk factor of false-negative and false-positive for T-SPOT.TB in active tuberculosis. J Clin Lab Anal. 2018;32(2). https://doi.org/10.1002/jcla.22273.
Shaikh N, Gupte A, Dharmshale S, Pokkali S, Thakar M, Upadhye VJ, et al. Novel interferon-gamma assays for diagnosing tuberculosis in young children in India. Int J Tuberc Lung Dis. 2017;21(4):412–9. https://doi.org/10.5588/ijtld.16.0428.
Ferrara G, Losi M, D’Amico R, Roversi P, Piro R, Meacci M, et al. Use in routine clinical practice of two commercial blood tests for diagnosis of infection with Mycobacterium tuberculosis: a prospective study. Lancet. 2006;367(9519):1328–34. https://doi.org/10.1016/S0140-6736(06)68579-6.
Seddon JA, Paton J, Nademi Z, Keane D, Williams B, Williams A, et al. The impact of BCG vaccination on tuberculin skin test responses in children is age dependent: evidence to be considered when screening children for tuberculosis infection. Thorax. 2016;71(10):932–9. https://doi.org/10.1136/thoraxjnl-2015-207687.
Acknowledgements
Not Applicable.
Funding
This project was supported by Taishan Scholar Project of Shandong Province (NO.tsqn202211358).
Author information
Authors and Affiliations
Contributions
YYH, ZYA, and WMS designed the study. HJ, WMS, and HY were involved in the literature review and screening, data analysis, interpretation. YYH and WMS wrote the paper. HJ revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
N/A.
Consent to participate
N/A.
Consent for publication
N/A.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, YH., Hou, J., He, Y. et al. Interferon-γ release assay and mantoux response in infants with tuberculous meningitis in low and intermediate burden countries. BMC Infect Dis 23, 364 (2023). https://doi.org/10.1186/s12879-023-08327-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08327-4