
Abstract
Background
Mycobacterium tuberculosis genotyping has been crucial to determining the distribution and impact of different families on disease clinical presentation. The aim of the study was to evaluate the associations among sociodemographic and clinical characteristics and M. tuberculosis lineages from patients with pulmonary tuberculosis in Orizaba, Veracruz, Mexico.
Methods
We analyzed data from 755 patients whose isolates were typified by 24-loci mycobacterial interspersed repetitive unit–variable number of tandem repeats (MIRU–VNTR). The associations among patient characteristics and sublineages found were evaluated using logistic regression analysis.
Results
Among M. tuberculosis isolates, 730/755 (96.6%) were assigned to eight sublineages of lineage 4 (Euro-American). Alcohol consumption (adjusted odds ratio [aOR] 1.528, 95% confidence interval (CI) 1.041–2.243; p = 0.030), diabetes mellitus type 2 (aOR 1.625, 95% CI 1.130–2.337; p = 0.009), sputum smear positivity grade (3+) (aOR 2.198, 95% CI 1.524–3.168; p < 0.001) and LAM sublineage isolates (aOR 1.023, 95% CI 1.023–2.333; p = 0.039) were associated with the presence of cavitations. Resistance to at least one drug (aOR 25.763, 95% CI 7.096–93.543; p < 0.001) and having isolates other than Haarlem and LAM sublineages (aOR 6.740, 95% CI 1.704–26.661; p = 0.007) were associated with treatment failure. In a second model, multidrug resistance was associated with treatment failure (aOR 31.497, 95% CI 5.119–193.815; p < 0.001). Having more than 6 years of formal education was not associated with treatment failure.
Conclusions
Knowing M. tuberculosis genetic diversity plays an essential role in disease development and outcomes, and could have important implications for guiding treatment and improving tuberculosis control.
Similar content being viewed by others


Background
The agent responsible for tuberculosis belongs to Mycobacterium tuberculosis complex (MTBC). Pulmonary tuberculosis is the most common disease presentation, reported in 4.8 million cases worldwide [1]. The state of Veracruz in southern Mexico reports the highest number of cases (2198) nationwide [2]. The incidence in the municipality of Orizaba, Veracruz was 16–38 cases/100,000 inhabitants during the period 1995–2010 surpassing the national incidence [3].
Nowadays, nine M. tuberculosis lineages have been identified strongly associated with particular geographic regions [4, 5]. In the Americas, tuberculosis is mainly caused by lineage 4 also known as Euro-American lineage [6].
Mycobacterium tuberculosis genotyping is important because it contributes to knowledge regarding its genetic diversity [7, 8]. The current gold standard for genotyping is mycobacterial interspersed repetitive unit–variable number of tandem repeat (MIRU–VNTR) method. Currently, MIRUs are used as markers for strains classification and sub-classification. For example, within the Latin American & Mediterranean (LAM) family, a single repeat of MIRU40 has been proposed as a marker of RDRio sub-lineage [9].
Risk factors related to M. tuberculosis genetics help in the early identification of patients infected with lineages associated with increased risk of treatment failure, relapse, drug resistance and death [10]. External risk factors associated with active tuberculosis development are poverty, overpopulation, overcrowding and malnutrition, in addition to comorbidities such as human immunodeficiency virus (HIV) coinfection, diabetes mellitus type 2 (DM2), chronic kidney failure, silicosis, immunosuppressive therapies and addictions such as smoking and drinking [11, 12].
In addition to host and environmental risk factors, tuberculosis epidemiology can also be influenced by M. tuberculosis genetic diversity [13]. Some lineages have shown differences in their virulence phenotypes, affecting transmissibility and pathogenesis and having implications in treatment outcomes and failure in the effectiveness of the BCG vaccine [6, 14].
The aim of this study was to evaluate the association among sociodemographic and clinical characteristics and M. tuberculosis lineages from isolates of patients with pulmonary tuberculosis obtained in a population-based study conducted in Orizaba, Veracruz, Mexico from 1995 to 2010.
Methods
Study population and data collection
Between March 1995 and April 2010, pulmonary tuberculosis cases passive search was carried out in people over 15 years of age who had respiratory symptoms for more than two weeks in 12 health jurisdictions municipality of Orizaba, Veracruz, Mexico. During this period, 1132 patients were diagnosed and for this study 612 M. tuberculosis isolates were recovered from a strain collection and 143 more from a DNA collection using samples from these patients. We used the population-based cohort data from patients diagnosed with pulmonary tuberculosis from August 1, 1997, to April 30, 2010. The study was approved by the Ethics Committee (Ref. No. 1515). All participating patients signed informed consent forms.
As part of the cohort investigation, isolates were genotyped by 24-loci MIRU–VNTR and susceptibility tests were performed as previously described [15]. LAM RDRio and RD115 sublineages were classified according to the presence of a single repeat in MIRU40 and MIRU02 respectively.
Definitions
The following sociodemographic variables were considered: sex, age, education level, dirt-floor home, and rural residence locality, nearest health center distance, social security access, and consumption of alcohol, tobacco and illicit drugs. DM2 and HIV diagnosis was also considered. Presence of acid-fast bacilli (AFB) in sputum samples information was considered and was graded as follows: 1 + (1–9 bacilli per 100 observed fields), 2 + (1–9 bacilli per 10 observed fields) or 3 + (1–9 bacilli per observed field). We included fever, hemoptysis and presence of cavitations variables, each used dichotomously. Body mass index (BMI) and number of days between symptom onset and start of treatment were calculated.
We used tuberculosis prevention and control program (NOM-SSA-006) operational definitions for treatment outcomes, except failure and death, which were defined according to international definitions [16, 17]: cure, patient who completed treatment, with signs and symptoms disappearance, or patient who had smear or culture negative at the end of treatment; failure, patient who had smear or culture positive after five months or later during treatment; and treatment completion, patient who completed his/her treatment regimen with signs and symptoms disappearance and smear or culture were not performed. Patients who did not complete treatment were classified into the following two categories: abandon, patient who interrupts treatment for 30 days or more; and death during treatment, patient who died due to any other cause during treatment.
Lineage variable was operationalized in disaggregated and aggregate way according to MIRU–VNTR genotyping. Disaggregated variable considers each identified sublineage, Haarlem, LAM, Cameroon, UgandaI, Ghana, S, X, TUR, EAI, Beijing and unknown. Aggregate variable considers lineage frequency, Haarlem, LAM and lineages other than Haarlem and LAM, because of the small frequency of each other lineages.
Statistical analysis
We calculated the distributions percentage for qualitative variables as well as medians and interquartile ranges (IQR) for quantitative variables. We used Pearson chi-square test for dichotomous variables, binomial test for categorical variables and Kruskal–Wallis test for quantitative variables. Unconditional logistic regression models were adjusted to explain treatment failure and the presence of cavitation on radiography. Two models were adjusted to explain treatment failure: one included resistance variable to at least one drug, and the other included MDR. To include variables in a multivariate model were considered those that in the bivariate analysis had values of p ≤ 0.20 and biological plausibility. We estimated adjusted odds ratio (aOR) and 95% confidence intervals (CIs).
Analyses were performed using STATA® v15 statistical software package (StataCorp LP, College Station, TX, USA).
Results
The characteristics of the studied patients are shown in Table 1. The proportion of individuals among the population examined was similar to the proportion represented by this same group. A total of 755 patients were included in the study, 442 (59%) of whom were men, with a median age of 45 years (IQR 32–59). There were 507 (67%) patients with more than six years of formal education, and 174 (23%) lived in dirt-floor homes. Comorbidity with DM2 was reported in 250 (33%) patients. HIV status was known for 739 patients, of whom 13 (2%) were positive. Resistance to any drug was present in 116/612 (19%) isolates, and 20 (3%) were MDR. The most common clinical findings were fever and cavitation in 531/752 (71%) and 282/626 (45%) patients respectively. Cure was recorded in 532/755 (70%) patients.
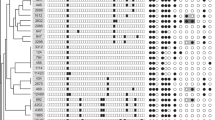
We identified ten sublineages among the 755 M. tuberculosis isolates (one from each patient) genotyped by 24-loci MIRU–VNTR. The most frequent sublineages were Haarlem (419, 55.5%) and LAM (163, 21.6%) which was sub classified in RDRio (114/163, 69.9%) characterized by one repeat in MIRU40 and RD115 (31/163, 19%) characterized by one repeat in MIRU02, followed by Cameroon (49, 6.5%), Uganda I (28, 3.7%), Ghana (23, 3%), S (18, 2.4%), X (15, 2%), TUR (15, 2%), EAI (15, 2%) and Beijing (2, 0.2%). It was not possible to determine lineage in eight isolates (1.1%) and therefore, these were considered unknown, the distribution of M. tuberculosis isolates in the jurisdiction of Orizaba, Veracruz is shown in Fig. 1.

Map of the distribution of M. tuberculosis isolates in the jurisdiction of Orizaba, Mexico
Data analysis revealed that Haarlem sublineage had the highest proportion (318/419, 75.9%) of clustered patients compared with other sublineages. Patients with Cameroon sublineage isolates had more days between symptom onset and start of treatment (median 129, IQR 83–198), and patients isolates with Ghana sublineage presented hemoptysis (11/23, 47.8%) with greater frequency compared with the other sublineages. EAI sublineage isolates were more frequent in men (12/15, 80.0%), in DM2 patients (10/15, 66.7%) and in patients who had ever smoked (7/15, 46.7%). Patients with Beijing sublineage isolates were older (median 59 years, IQR 57–60) than patients with other sublineages; one of the two patients had HIV (1/2, 50%), the other had DM2 besides the isolate was MDR (1/2, 50%), both showed higher BMI (median 25.4, IQR 21.6–29.3) compared to patients with other sublineages (Additional file 1: Table S1).
The possible association between sublineages and population clinical characteristics was explored, grouping patients with Haarlem, LAM and lineages other than Haarlem and LAM (Table 2). Significantly, most of the patients with Haarlem lineage were men (61.3%, 247/419); 25.4% (106/417) had ever smoked, had a median BMI of 20.5 (IQR 18.1–23.4), lower than the average, and 75.9% (318/419) were found clustered (p < 0.05). Significantly more patients with LAM lineage presented cavitation 54.5% (74/136) as radiographic finding (p = 0.023). In patients with sublineages other than Haarlem and LAM 40.5% (70/173) had hemoptysis as the most common clinical feature (p = 0.005).
Regarding treatment outcomes, we compared cure or treatment completion with treatment failure in all identified lineages. It was observed that patients with X sublineage isolates (2/11, 18.2%) and unknown isolates (1/7, 14.3%) had the highest failure rates, followed by Cameroon (3/41, 7.3%), EAI (1/15, 6.7%), S (1/18, 5.6%), LAM (6/135, 4.4%), Uganda I (1/26, 3.9%) and Haarlem (5/358, 1.4%). Patients with Beijing, Ghana and TUR lineages did not experience treatment failure (Additional file 1: Table S2).
Treatment outcome according to sublineage is summarized in Additional file 1: Table S3. When comparing cure or completion with treatment failure, patients with sublineages other than Haarlem and LAM showed higher proportion of treatment failure (9/152, 5.9%) than patients with Haarlem (1.4%) and LAM (4.4%) lineages (p = 0.016).
The comparison among clinical characteristics according to cure or treatment completion compared to failure, revealed higher proportion of treatment failure in patients who had ever smoked (8/20, 40% vs 131/624, 21.0%; p = 0.034), showed resistance to at least one drug (13/17, 76.0% vs 80/505, 16.0%; p < 0.001), showed MDR presence (5/17, 2.0% vs 6/505, 1.0%, p < 0.001) and had sublineages other than Haarlem and LAM (9/20, 45.0% vs 143/625, 23.0%; p = 0.022) (Table 3). We observed higher proportion of cure in patients who had formal education > 6 years (423/625, 68.0% vs 9/20, 45%; p = 0.034), had Haarlem sublineage (353/625, 56.5% vs 5/20, 25%; p = 0.005) and presented LAM RDRio sublineage (1/6, 16.7% vs 92/129, 71.3%; p = 0.005).
We compared cavitation presence or absence with population clinical characteristics (Table 4). We found that patients with cavitation had DM2 as comorbidity (106/282, 38.0% vs 95/344, 28.0%; p = 0.008), presented greater number of AFB in sputum samples (101/282, 36.0% vs 71/344, 21.0%, p < 0.001) and presented LAM sublineage isolates (74/282, 26.2% vs 62/344, 18.0%; p = 0.013).
Using logistic regression models, we performed two adjusted models to explain treatment failure compared to cure and treatment completion; in one we included resistance variable to at least one drug, and in the other we included MDR variable (Table 5). In the first model adjusted for covariates, treatment failure was associated with resistance to at least one drug (aOR 25.763, 95% CI 7.096–93.543; p < 0.001) and having lineage other than Haarlem and LAM (aOR 6.740, 95% CI 1.704–26.661; p = 0.007). In the model that included MDR variable adjusted for covariates, failure was associated with MDR (aOR 31.497, 95% CI 5.119–193.815; p < 0.001), in both models having > 6 years of formal education was not associated with treatment failure (aOR 0.166, 95% CI 0.045–0.615; p = 0.007), (aOR 0.248, 95% CI 0.069–0.885; p = 0.032) respectively.
We performed an adjusted logistic regression model to identify variables associated with cavitations presence (Table 6). Cavitation presence was associated with having ever consumed alcohol (aOR 1.528, 95% CI 1.041–2.243; p = 0.030), having DM2 (aOR 1.625, 95% CI 1.130–2.337; p = 0.009), AFB sputum positivity grade of 3 + (aOR 2.198, 95% CI 1.524–3.168; p < 0.001) and having the LAM sublineage (aOR 1.023, 95% CI 1.023–2.333; p = 0.039).
Discussion
This study describes the association among clinical and sociodemographic characteristics of patients with pulmonary tuberculosis and little described M. tuberculosis sublineages lineage 4 in the health jurisdiction of Orizaba, Veracruz, Mexico between 1995 and 2010. Our study population presented high frequency of lineage 4, Euro-American isolates. In addition, associated characteristics with treatment failure and cavitation presence were identified.
In this study, lineage 4 (Euro-American) was the most common (~ 96%) lineage identified, consistent with previous reports that have shown that isolates with this lineage are predominant in Mexico [18]. We were also able to observe that isolates with LAM lineage (163), the proportion of RDRio was 69.9%, higher compared to the 63.1% recently described in isolates from Northern Mexico and in isolates from Venezuela (55%), Argentine (11%) and Paraguay (10%) [19, 20]. Therefore, our results support that these lineages are endemic and that strains spread regionally with different rates of distribution.
We found that compared with other sublineages, cases with Haarlem sublineage isolates had higher proportion of clustered patients. A previous study showed similar results; the authors found that Haarlem sublineage isolates were more likely to belong to clusters [21]. This result confirms the wide distribution and genetic diversity of lineage 4 due to its virulence, which is reflected in cluster formation and its transmission success among the population [22].
On the other hand, we found that patients with Cameroon sublineage isolates showed more days between symptom onset and treatment start. Similar result have been described in patients with lineage 7 isolates in Ethiopia, where the time was longer between symptom onset and treatment start was attributed to lineage 7 strains slow growth [21]. Because treatment initiation is important to cut transmission chains, it is necessary to phenotypically confirm Cameroon sublineage isolates growth rate. To confirm this hypothesis, we cultured 45 isolates with Cameroon lineage on MGIT medium and determined the time and units of growth. We observed, that the Cameroon isolates grew less (14.6 CFU/h) compared to H37Rv (24.7 CFU/h).
Respect to Ghana sublineage, we found the majority of patients presented haemoptysis; this finding has not been reported thus far in literature. However, more data are needed.
Another interesting result was that cases with isolates of EAI lineage were more frequent in men, in patients with DM2 and patients who had ever smoked. It has been described that DM2 alone is associated with M. tuberculosis infection and progression to active disease with severe disease presentation [23]. Furthermore, decreased lung function has been observed in smokers with DM2 compared to nonsmokers [24]. Therefore, it is likely that social factors contribute to EAI dissemination, also these patients showed higher cavitations proportion (69.2%), without statistical significance. Previously, a study that evaluated host–pathogen relationship and its association with clinical outcomes in patients with tuberculosis described that patients infected with strains that originated in geographic regions other than the patient’s origin (allopatric) such as EAI lineage in America presented an increased lung damage risk [25]. As observed in our results, it has been suggested that although these lineages are less adapted to transmit and cause disease in fully competent members of allopatric human populations, they can do so in the context of impaired host immune resistance [26]. However, it would be necessary to perform whole genome sequence on EAI lineage isolates to determine pathogen genetic characteristics that facilitate its possible adaptation to the host and transmission.
Furthermore, East Asia (Beijing) lineage was found in two elderly patients, one of them had HIV and the other had DM2 and MDR. Beijing isolates were genetically distinct, with 9/15 different alleles by 24-loci MIRU–VNTR; these cases were probably due to reactivation. MDR has been associated with Beijing family; however, in this study, data are not conclusive because there were only two isolates [11, 27]. However, it is very likely that MDR isolate is due to antibiotics selective pressure because patient had received treatment previously.
We also observed higher proportion of treatment failure in patients with isolates of sublineages other than Haarlem and LAM, in patients who had ever smoked and in patients with isolates resistant to at least one drug or MDR. A greater proportion of resistance was found in Cameroon (13/49, 30.2%), UgandaI (5/22, 22.7%) and Ghana (2/16, 12.5%) sublineage isolates. A recent study conducted in Niger reported that 75% of Cameroon and Ghana sublineage isolates were resistant to RIF and MDR [28]. However, treatment failure could be also the result of "antibiotic resilience" as recently described by Quingyun et al., they found that mutations in resR (Rv1830) gene do not show canonical drug resistance or drug tolerance but instead shorten the post-antibiotic effect, meaning that they enable M. tuberculosis to resume growth after drug exposure substantially faster than wild-type strains, and these mutations are associated to treatment failure acting in a regulatory cascade with other transcription factors controlling cell growth and division. Furthermore, they described that up to 10% of strains from high-tuberculosis-burden countries showed fixed mutations in these regions [29].According to our results Cameroon and Ghana sublineages geographically restricted within Euro-American lineage, seem to have adapted to the study population and contribute significantly to the resistance generation and treatment failure. Therefore, it is necessary to genotype a greater number of isolates and performs susceptibility tests to determine the real impact on the resistance of lineages little described in Mexico and to perform whole genome sequencing to explore the possible association between resR mutation, treatment failure and whether any lineage is prone to acquire it.
Interestingly, having > 6 years of formal education was not associated with treatment failure. We believe that having higher education level probably implies that patients better understand treatment adherence and completion importance.
The LAM RDRio lineage has been described in other Latin American countries where it has been associated with the presence of cavitations, increased transmissibility and MDR [19]. However, in the present study we observed more proportion of LAM RDRio isolates in cured patients, previously in this study population was obtained that previous treatment (aOR 9.05, 95% CI 3.6–22.5, p < 0.001) and LAM lineage (aOR 4.25, 95% CI 1.4–12.7, p = 0.010) were associated with tuberculosis MDR [15]. These results have important implications in the tuberculosis control program, although isolates with LAM RDRio sub lineage are more prone to develop MDR following a previous treatment, patients seem to respond favorably to the second treatment.
Cavitations presence was associated with LAM sublineage, alcohol consumption, DM2 and AFB positivity grade 3+ . Similar results have been previously described regarding the presence of more severe manifestations in patients with DM2 and tuberculosis [30, 31]. Moreover, it has been reported that cavitations presence in pulmonary tuberculosis is associated with higher contagiousness/transmissibility due to high AFB load [32]. In addition, these results support those described by Pasopanodya et al., who report that modern lineages strains, such as Euro-American lineages, developed nonlethal properties; however, they cause lung damage, which increases their dissemination capacity among the population [25]. Therefore, the increase in the number of people with DM2 in Mexico could result in greater transmission of tuberculosis due to lung damage associated with the presence of LAM sublineage. We thus suggest implementing genotyping of M. tuberculosis isolates with the use of 24-loci MIRU–VNTR in Mexico and determining the impact of LAM sublineage.
In conclusion, this study provides relevant results in relation to the association between the presence of cavitations, comorbidities and LAM sublineage isolates. Additionally, treatment failure associated with sublineages other than Haarlem and LAM. Furthermore, we found the possible EAI sublineage isolates association in patients with DM2 and cavitation. We describe that the genetic diversity of M. tuberculosis lineage 4 (Euro-American) probably plays an essential role in disease presentation, which could have important implications for treatment management and to improve tuberculosis control in Mexico.
Availability of data and materials
The datasets used during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- aOR:
-
Adjusted odds ratio
- AFB:
-
Acid-fast bacilli
- BMI:
-
Body mass index
- CIs:
-
Confidence intervals
- DM2:
-
Diabetes mellitus type 2
- EMB:
-
Ethambutol
- HIV:
-
Human immunodeficiency virus
- INH:
-
Isoniazide
- IQR:
-
Interquartile ranges
- LAM:
-
Latin American & Mediterranean
- MDR-TB:
-
Tuberculosis multidrug-resistant
- MIRU–VNTR:
-
Variable number tandem repeat–mycobaterial interspersed repetitive unit
- MTBC:
-
Mycobacterium tuberculosis complex
- RIF:
-
Rifampicin
- STR:
-
Streptomycin
References
World Health Organization. Global tuberculosis report 2021. https://www.who.int/publications/i/item/9789240037021.
CENAPRECE, 2022. Programas Preventivos. Direccion de Micobacteriosis. Casos Nuevos de Tuberculosis Pulmonar. Estados Unidos Mexicanos 1990–2016. http://www.cenaprece.salud.gob.mx/programas/interior/micobacteriosis/tuberculosis/cifras_oficiales.html.
Blanco-Guillot F, Castaheda-Cediel ML, Cruz-Hervert P, Ferreyra-Reyes L, Delgado-Sanchez G, Ferreira-Guerrero E, et al. Genotyping and spatial analysis of pulmonary tuberculosis and diabetes cases in the state of Veracruz, Mexico. PLoS ONE. 2018;13(3): e0193911.
Coll F, McNerney R, Guerra-Assunção JA, Glynn JR, Perdigão J, Viveiros M, et al. A robust SNP barcode for typing Mycobacterium tuberculosis complex strains. Nat Commun. 2014;5:4812.
Coscolla M, Gagneux S, Menardo F, Loiseau C, Ruiz-Rodriguez P, Brites D. Phylogenomics of Mycobacterium africanum reveals a new lineage and a complex evolutionary history. Microb Genom. 2021;7(2): 000477.
Gagneux S. Host-pathogen coevolution in human tuberculosis. Philos Trans R Soc Lond B Biol Sci. 2012;367(1590):850–9.
Kato-Maeda M, Metcalfe JZ, Flores L. Genotyping of Mycobacterium tuberculosis: application in epidemiologic studies. Future Microbiol. 2011;6(2):203–16.
Couvin D, Rastogi N. Tuberculosis—a global emergency: tools and methods to monitor, understand, and control the epidemic with specific example of the Beijing lineage. Tuberculosis. 2015. https://doi.org/10.1016/j.tube.2015.02.023.
Mokrousov I, Vyazovaya A, Iwamoto T, Skiba Y, Pole I, Zhdanova S, et al. Latin–American–Mediterranean lineage of Mycobacterium tuberculosis: human traces across pathogen’s phylogeography. Mol Phylogenet Evol. 2016;99:133–43.
Wiens KE, Woyczynski LP, Ledesma JR, Ross JM, Zenteno-Cuevas R, Goodridge A, et al. Global variation in bacterial strains that cause tuberculosis disease: a systematic review and meta-analysis. BMC Med. 2018;16(1):1–13.
Gagneux S. Ecology and evolution of Mycobacterium tuberculosis. Nat Rev Microbiol. 2018;16(4):202–13.
Dheda K, Barry CE, Maartens G. Tuberculosis. Lancet. 2016;387:1211–26.
Chae H, Shin SJ. Importance of differential identification of Mycobacterium tuberculosis strains for understanding differences in their prevalence, treatment efficacy, and vaccine development. J Microbiol. 2018;56(5):300–11.
Coscolla M, Gagneux S. Consequences of genomic diversity in Mycobacterium tuberculosis. Semin Immunol. 2014;26(6):431–44.
Ordaz-Vázquez A, Torres-González P, Cruz-Hervert P, Ferreyra-Reyes L, Delgado-Sánchez G, García-García L, et al. Genetic diversity and primary drug resistance transmission in Mycobacterium tuberculosis in southern Mexico. Infect Genet Evol. 2021;93: 104994.
NORMA Oficial Mexicana NOM-006-SSA2-1993, para la Prevención y control de la tuberculosis.
Varaine F, Rich M (eds). Tuberculosis: practical guide for clinicians, nurses, laboratory technicians and medical auxiliaries. Médecins San Frontières and Partners In Health; 2014.
Flores-Treviño S, Mendoza-Olazarán S, Garza-González E. Drug resistance and molecular epidemiology of Mycobacterium tuberculosis in Mexico: a systematic review. Salud Publica Mex. 2014;56(1):63–77.
Bocanegra-García V, Cortez-de-la-Fuente LJ, Nakamura-López Y, González GM, Rivera G, Palma-Nicolás JP. RDRio Mycobacterium tuberculosis strains associated with isoniazid resistance in Northern Mexico. Enferm Infecc Microbiol Clin. 2021;39(8):399–402.
DíazAcosta CC, Russomando G, Candia N, Ritacco V, Vasconcellos SEG, De BerrêdoPinhoMoreira M, et al. Exploring the “Latin American Mediterranean” family and the RDRio lineage in Mycobacterium tuberculosis isolates from Paraguay, Argentina and Venezuela. BMC Microbiol. 2019;19(1):131.
Yimer SA, Norheim G, Namouchi A, Zegeye ED, Kinander W, Tønjum T, et al. Mycobacterium tuberculosis lineage 7 strains are associated with prolonged patient delay in seeking treatment for pulmonary tuberculosis in Amhara region, Ethiopia. J Clin Microbiol. 2015;53(4):1301–9.
Stucki D, Brites D, Jeljeli L, Coscolla M, Liu Q, Trauner A, et al. Mycobacterium tuberculosis lineage 4 comprises globally distributed and geographically restricted sublineages. Nat Genet. 2016;48(12):1535–43.
Restrepo BI, Schlesinger LS. Host-pathogen interactions in tuberculosis patients with type 2 diabetes mellitus. Tuberculosis. 2013. https://doi.org/10.1016/S1472-9792(13)70004-0.
Kolahian S, Leiss V, Nürnberg B. Diabetic lung disease: fact or fiction? Rev Endocr Metab Disord. 2019;20(3):303–19.
Pasipanodya JG, Moonan PK, Vecino E, Miller TL, Fernandez M, Slocum P, et al. Allopatric tuberculosis host–pathogen relationships are associated with greater pulmonary impairment. Infect Genet Evol. 2013;16:433–40.
Gagneux S, DeRiemer K, Van T, Kato-Maeda M, De Jong BC, Narayanan S, et al. Variable host-pathogen compatibility in Mycobacterium tuberculosis. Proc Natl Acad Sci USA. 2006;103(8):2869–73.
Hu Y, Ma X, Graviss EA, Wang W, Jiang W, Xu B. A major subgroup of Beijing family Mycobacterium tuberculosis is associated with multidrug resistance and increased transmissibility. Epidemiol Infect. 2011;139(1):130–8.
Ejo M, Hassane-Harouna S, Souleymane MB, Lempens P, Dockx J, Uwizeye C, et al. Multidrug-resistant patients receiving treatment in Niger who are infected with M. tuberculosis Cameroon family convert faster in smear and culture than those with M. tuberculosis Ghana family. Tuberculosis. 2020;122:101922.
Liu Q, Zhu J, Dulberger CL, Stanley S, Wilson S, Chung ES, et al. Tuberculosis treatment failure associated with evolution of antibiotic resilience. Science. 2022;378(6624):1111–8.
Jiménez-Corona ME, Cruz-Hervert LP, García-García L, Ferreyra-Reyes L, Delgado-Sánchez G, Bobadilla-Del-Valle M, et al. Association of diabetes and tuberculosis: impact on treatment and post-treatment outcomes. Thorax. 2013;68(3):214–20.
Armstrong LR, Steve Kammerer J, Haddad MB. Diabetes mellitus among adults with tuberculosis in the USA, 2010–2017. BMJ Open Diabetes Res Care. 2020;8(1): e001275.
Palaci M, Dietze R, Hadad DJ, Ribeiro FKC, Peres RL, Vinhas SA, et al. Cavitary disease and quantitative sputum bacillary load in cases of pulmonary tuberculosis. J Clin Microbiol. 2007;45(12):4064–6.
Acknowledgements
All patients who participated in the study and staff personal.
Funding
This work was supported (Grant Number: 233506) by the Consejo Nacional de Ciencia y Tecnologia (https://www.conacyt.gob.mx).
Author information
Authors and Affiliations
Contributions
MBV, PTG, LGG, APDL and JSO designed the study. AOV performed the experiments. LFR and SCQ acquired field data. AOV, MBV and GDS performed data analysis and interpretation. GDS provided the statistical analysis. AOV and MBV drafted the initial manuscript. LGG, APDL and JSO revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Research was conducted according to the guiding principles of the Declaration of Helsinki. Participants provided written informed consent to participate in this study. The study was approved by the Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran institutional ethics and research committees (Ref. No. 1515; July 15th 2015). All participants were referred to health facilities to receive treatment in accordance with the stipulations of the National Program for the Prevention and Control of TB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Table S1. Sociodemographic and clinical characteristics of patients with pulmonary tuberculosis according to disaggregated sublineage, determined by 24-loci MIRU-VNTR, Orizaba Veracruz 1997-2010 (n=755). Table S2. Treatment outcome of patients with pulmonary tuberculosis according to disaggregated lineage by 24-loci MIRU-VNTR, Orizaba Veracruz 1997-2010 (n=755). Table S3. Treatment outcome of patients with pulmonary tuberculosis according to aggregated lineage by 24-loci MIRU-VNTR, Orizaba Veracruz 1997-2010 (n=755).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ordaz-Vázquez, A., Torres-González, P., Ferreyra-Reyes, L. et al. Mycobacterium tuberculosis lineage 4 associated with cavitations and treatment failure. BMC Infect Dis 23, 154 (2023). https://doi.org/10.1186/s12879-023-08055-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08055-9