
Abstract
Background
Invasive pneumococcal disease is a major cause of infant morbidity and death worldwide. Vitamin D promotes anti-pneumococcal immune responses in vitro, but whether improvements in infant vitamin D status modify risks of nasal pneumococcal acquisition in early life is not known.
Methods
This is a secondary analysis of data collected in a trial cohort in Dhaka, Bangladesh. Acute respiratory infection (ARI) surveillance was conducted from 0 to 6 months of age among 1060 infants of women randomized to one of four pre/post-partum vitamin D dose combinations or placebo. Nasal swab samples were collected based on standardized ARI criteria, and pneumococcal DNA quantified by qPCR. Hazards ratios of pneumococcal acquisition and carriage dynamics were estimated using interval-censored survival and multi-state modelling.
Results
Pneumococcal carriage was detected at least once in 90% of infants by 6 months of age; overall, 69% of swabs were positive (2616/3792). There were no differences between any vitamin D group and placebo in the hazards of pneumococcal acquisition, carriage dynamics, or carriage density (p > 0.05 for all comparisons).
Conclusion
Despite in vitro data suggesting that vitamin D promoted immune responses against pneumococcus, improvements in postnatal vitamin D status did not reduce the rate, alter age of onset, or change dynamics of nasal pneumococcal colonization in early infancy.
Trial registration Registered in ClinicalTrials.gov with the registration number of NCT02388516 and first posted on March 17, 2015.
Similar content being viewed by others


Background
Streptococcus pneumoniae (pneumococcus) is one of the leading bacterial causes of meningitis, sepsis, pneumonia and otitis media in young children worldwide, with the burden falling on low- and middle-income countries (LMICs) [1]. Pneumococcus is not a common cause of neonatal infection in high-income countries, but a study of neonatal infections in South Asia identified pneumococcus as a culture-confirmed cause of neonatal sepsis almost as commonly as Streptococcus agalactiae (group B streptococcus) in infants 0–59 days of age [2]. A 2011 review reported pneumococcus accounting for 6% of pathogenic bacteria isolated among cases of community-acquired neonatal sepsis in LMICs [3].
One or more serotypes of pneumococcus typically colonize the nasopharynx in childhood [4, 5]. Ongoing colonization (‘carriage’) is the presence of pneumococcus on a mucosal surface without tissue invasion or damage. Onset of colonization by a serotype (‘acquisition’) may occur as early as the immediate postnatal period; however, carriage status in an individual can change over time (‘carriage dynamics’), therefore an individual may be colonized by multiple serotypes concurrently, and some serotypes may persist long-term while others are lost and replaced by different serotypes [5,6,7,8]. Carriage is asymptomatic but can be an antecedent to otitis media and invasive pneumococcal disease (IPD), usually attributable to a recently acquired serotype [9]. Factors influencing progression from carriage to disease include the virulence of the colonizing serotype (certain serotypes are more likely to cause IPD), respiratory virus co-infections, and host immune status [6,7,8].
Introduction of pneumococcal conjugate vaccines (PCV), which protect against the most common IPD-causing serotypes, has substantially reduced the carriage rates of vaccine-specific serotypes and lowered the incidence of vaccine serotype-related otitis media and IPD; however, overall rates of nasopharyngeal colonization have not decreased owing to the replacement of vaccine-specific serotypes with non-vaccine serotypes [10,11,12]. Disease occurs most commonly due to recently acquired serotypes in the nasopharynx [9]. Thus, carriage is often used as a trial endpoint with acquisition being of particular interest [13]. Since vaccine studies show the prevention of acquisition of vaccine serotypes reduces the risk of IPD, delaying early-life nasopharyngeal acquisition of all serotypes may reduce the overall infant IPD burden. High pneumococcal density (bacterial load of pneumococcus in the nasopharynx) is associated with lower respiratory tract infections (LRTI) and pediatric pneumonia [14]. Mouse models also show increasing pneumococcal density in the nasal cavity facilitates pneumococcal transmission to susceptible mice [15]. Since PCV vaccination does not begin before 6 weeks of age and infants remain unprotected against several vaccine serotypes until after their second dose (typically given at 10 weeks in many LMICs) [16,17,18], alternative strategies may reduce IPD risk in the first few months of life.
Vitamin D (VD) supplementation is a candidate preventive intervention against IPD based on its observed anti-pneumococcal effects in in vitro studies where VD stimulated maturation of dendritic cells, reduced pro-inflammatory cytokines, and increased pneumococcal killing [19,20,21]. However, studies examining the effect of prenatal VD supplementation on newborn immune function produced inconsistent results [22,23,24,25]. Observational studies in children found VD insufficiency and deficiency associated with longer recovery times from pneumonia, increased pneumonia severity and increased risk of acute respiratory infections (ARI) [26,27,28,29]. Yet, results from randomized controlled trials of VD supplementation as a prevention or treatment method for ARI in children are mixed [30,31,32,33]. No studies directly addressed whether VD affects pneumococcal carriage in young children. A postnatal delay in nasopharyngeal pneumococcal acquisition due to improved maternal-infant VD status could be beneficial in reducing the risk of early-infant IPD.
Bangladesh is a LMIC with a high burden of IPD [34] and a high prevalence of maternal and neonatal VD deficiency [35]. In this sub-study of a randomized controlled trial and nested cohort study in Bangladesh [33, 35], we aimed to estimate the dose-dependent effect of maternal VD supplementation during pregnancy and lactation on the risk of nasal pneumococcal acquisition, carriage dynamics (cycling between negative and positive carriage) and nasal pneumococcal carriage density (copies/mL) in infants from birth to 6 months of age.
Methods
Study design and participants
This was a secondary analysis of data collected during the Maternal Vitamin D Supplementation to Prevent Acute Respiratory Infections (MDARI) study nested in the Maternal Vitamin D for Infant Growth (MDIG) trial (ClinicalTrials.gov:NCT02388516; First Registered: 17/03/2015). The MDIG trial was a randomized, double-blind, placebo-controlled trial of VD supplementation in pregnancy and the first 6 months postpartum conducted in Dhaka, Bangladesh, where generally healthy women at 17–24 weeks of gestation were randomly assigned to receive 1 of 5 weekly VD supplementation doses: 0 IU during pregnancy and postpartum (group A); 4200 IU (B), 16,800 IU (C) or 28,000 IU during pregnancy only (D); and 28,000 IU during pregnancy and up to 26 weeks postpartum (E). Written informed consent was obtained from all women for participation in the MDIG and MDARI studies, including consent for storage and use of biological specimens. Detailed methods and primary results of the MDIG trial and MDARI study were previously described [33, 35, 36]. The MDARI study was approved by research ethics committees at the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) (ERC protocol PR-14079), and as a MDIG sub-study at the Hospital for Sick Children in Toronto (REB 100039072). All methods were carried out in accordance with relevant guidelines and regulations. The MDARI protocol included pneumococcal carriage detection procedures and a pre-specified aim to examine effects of maternal vitamin D supplementation on infant pneumococcal carriage; however, the aims and statistical analysis plan for the sub-study described in this paper were further developed and finalized after trial data collection and laboratory analyses were completed.
Data collection methods
Infant ARI episodes were monitored by active and passive surveillance from birth to 6 months, as described previously [33, 35, 36]. Infants with signs of ARI or other illness detected during routine home visits were referred to study physicians for further assessment. Parents were counseled to contact study personnel if infants had signs of ARI (e.g., difficulty breathing, cough, nasal congestion, runny nose, hot to the touch) or were taken to hospital. Collection of a nasal swab specimen was routinely performed when ARI criteria were ascertained beyond the 1st week of life (Additional file 1: Table S1), and/or hospitalization with a diagnosis of pneumonia or bronchiolitis occurred (preferentially during hospitalization or otherwise within 7 days of discharge). Among infants with clinical ARI, a nasal swab was collected if another nasal swab had not been collected in the preceding 7 days and one of these criteria were met: there was at least one study visit in the preceding surveillance week where clinical criteria for ARI were not met, ARI features worsened clinically (i.e., upper respiratory tract infection in the preceding week was classified as a LRTI in the current week), or at least four study weeks passed since the last nasal swab collection. Nasal epithelial cells were collected using a sterile nasal flocked swab (Copan Diagnostics, Inc., model number 56780CS01) stored in universal transport medium (Copan Diagnostics, Inc.) and transported to the Virology Lab at icddr,b in an insulated cold bag. Samples were stored at − 80 °C until batched nucleic acid extraction. Nasal swab specimens were collected between December 2014 and August 2016. The ten-valent PCV vaccine (PCV10) was introduced into the routine immunization schedule of Bangladesh in March 2015. Infants were eligible for inclusion in this sub-study if at least 1 nasal swab was collected over the observation period. All swabs collected during the 6-month surveillance period, including those collected during the 1st week of life, were included in this sub-study analysis.
Total nucleic acids were extracted from the nasal swab transport medium using the InviMag Pathogen Kit/KF96 (Invitek Molecular, Berlin, Germany) on the Kingfisher Flex 96 (Thermo Fisher Scientific). Extracted nucleic acid was a template for quantification of pneumococcal copy number by real-time PCR amplification of lytA, a single-copy gene specific to S. pneumoniae strains. The qPCR assays were carried out using the TaqMan™ Gene Expression Master Mix (Applied Biosystems™, Thermo Fisher Scientific), forward primer ACGCAATCTAGCAGATGAAGCA, reverse primer TCGTGCGTTTTAATTCCAGCT, and probe FAM TGCCGAAAACGCTTGATACAGGGAG-MGB. Each 25 µL reaction contained 10 µL nucleic acid template, 12.5 µL master mix, 0.5 µL of 10 µM stock solutions of each of the primers and probe, and 1 µL water. Real time PCR was conducted using the following thermal conditions in an ABI 7500 (Applied Biosystem, USA): 95 °C for 10 min followed by 40 cycles of 95 °C for 15 s and 60 °C for 1 min. Quality of amplification was confirmed by visual inspection of the Ct curve; if the quality of the amplification was suboptimal, the test was repeated or considered negative. Conversions of Ct values to copies/mL (carriage density) were based on standard curves generated by determining the threshold cycle values for DNA templates containing lytA. All standards were performed in triplicate, and a negative (no template) and positive (lytA plasmid control) control were included in every run. All amplification curves were manually inspected. A sample was considered positive for pneumococcus if the Ct value was < 35 or was ≤ 38 and showed appropriate amplification upon visual inspection of the Ct curve (i.e., sigmoidal shape).
Serum 25-hydroxyvitamin D (25(OH)D) concentration was measured, as described, in blood samples collected from the mother at delivery and 3-months postpartum, cord blood, and from infants at 3 months [35].
Statistical analysis
The effect of maternal VD supplementation on the rate of initial nasal pneumococcal acquisition in infants was estimated using interval-censored survival modelling assuming initial pneumococcal acquisition occurred in the interval from birth to a positive swab (if the first swab was positive) or in the interval between a negative swab and the first positive swab. The primary analysis included all infants with at least one swab collected, and otherwise applied the intent-to-treat principle. In primary models, day 0 was the earliest entry point for infants, and all infants were assumed to be carriage-negative on day 0. The parametric model was fit to the data and the best fitting underlying parametric distribution (Gompertz) was chosen based on the Akaike’s Information Criterion, goodness of fit plots and the smooth hazard distribution of the placebo group (expected to provide the baseline hazard distribution). The timing and duration of the interval was based on the time of the infant’s first positive swab and the timing of their negative swabs (Additional file 6: Method S1). Results were expressed as hazard ratios (HR) with 95% confidence intervals (95%CI) and the placebo group was the reference group in all analyses.
Effects of maternal VD supplementation on infant nasal pneumococcal carriage dynamics were estimated using a multi-state model composed of two states: negative (pneumococcus absent) and positive (pneumococcus present). All infants were assumed to be negative for pneumococcal carriage at birth (day 0). Each ‘carriage episode’ represented the time spent in one state from when one swab result was generated until the next swab (or censoring). The multi-state model was used to estimate the probability of an infant being in a positive state at day 189 postnatal age (end of scheduled follow-up period) given negative starting state, total average length of time spent in each state, the expected time until an infant’s first positive episode, the HR of switching states in each VD supplementation group versus placebo and the ratio of the likelihood of transitioning from a positive-to-negative state versus negative-to-positive state. The multi-state model utilized a constant transition rate with a constant baseline hazard accounting for interval censoring.
Positive carriage density data were log-transformed due to the right-skewed distribution. The effect of maternal VD supplementation on log-transformed nasal pneumococcal carriage density (log-copies/mL) was examined using linear regression including only the swabs classified as “positive” for carriage. Generalized estimating equations (GEE) and robust standard errors accounted for multiple swabs from the same infant.
Sensitivity analyses tested the robustness of all primary analyses including variations of model fit and model variation including a sensitivity analysis where all infants were assumed carriage-negative at day 7 since infants were not considered at-risk of ARI during the first postnatal week in the MDARI study [33]. To test the robustness of the parametric interval-censored modelling, a Cox Proportional Hazard Model sensitivity test was completed. Analyses were performed using STATA version 15.1 and the msm package in R (version 3.4.2) was used for multi-state modeling.
Results
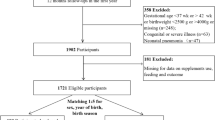
Of 1174 infants enrolled in the MDARI study, 1060 had at least one nasal swab and were eligible for inclusion in this sub-study (Fig. 1).

Vitamin D Interventions for Trial Arms and Enrolment of Eligible Infants for Sub-Studies1. 1Inclusion in current sub-study required the infant to have at least 1 swab taken during the study period. The inclusion/exclusion criteria for the MDIG & MDARI studies have been published elsewhere
Consistent with findings reported for the MDIG cohort [35], maternal and household characteristics at MDARI study enrolment were similar across the VD or placebo groups. There were VD dose-dependent differences in serum 25(OH)D concentration among mothers at delivery and 3 months postpartum (Table 1) and in cord and infant 3-month samples (Table 1), as reported for the MDIG cohort [35]. Other infant characteristics were similar across groups (Table 1).
Of 3792 nasal swab specimens collected, 69% (2616) tested positive for pneumococcus. Overall, 90% (949/1060) of infants were carriage-positive at least once during the first 6 months of life and the number of positive swabs increased with age (Fig. 2).

Weekly number and proportion of nasal swabs positive for pneumococcal carriage in infants up to 6 months of age in the MDARI cohort, including all maternal vitamin D supplementation groups (N = 1060)
The total numbers of swabs and proportions positive were similar across VD supplementation groups: 68% (500/737) in Group A, 66% (502/761) in Group B, 70% (507/798) in Group C, 71% (555/781) in Group D and 70% (499/715) in Group E. There was no significant effect of any dose of maternal VD supplementation during pregnancy and postpartum on the relative hazard of pneumococcal acquisition compared to placebo. The median age at first detection of pneumococcal carriage and was similar across intervention groups, ranging from 6.3 to 8.1 weeks (Table 2).
There was no significant effect of maternal VD supplementation during pregnancy and postpartum on infant pneumococcal density for any VD supplementation group compared to placebo (Table 2).
Metrics of nasal pneumococcal carriage dynamics based on multi-state modeling were similar across the VD and placebo groups (Table 3). Specifically, there was no significant effect of VD supplementation on the relative hazard of transitioning from a negative to positive carriage episode or from a positive to negative carriage episode (Table 3). The overall time spent positive across all carriage positive events was similar across the groups, ranging from between 115 to 125 days (Table 3). Among all intervention groups, the probability of pneumococcal carriage was high such that by 120 days of age, there was a 75% probability of a swab being positive (Additional file 7: Fig. S1). The ratio of the risk of progression to positive episode versus recovery from positive episode showed an increasing trend as the VD supplementation dosage increased but confidence intervals overlapped (Table 3).
All sensitivity analyses supported the findings of the primary analyses in demonstrating a lack of any significant effects of maternal VD supplementation on pneumococcal carriage acquisition, dynamics or density (Additional file 2: Table S2; Additional file 3: Table S3; Additional file 4: Table S4; Additional file 5: Table S5).
Discussion
In this sub-study of a randomized placebo-controlled dose-ranging trial in Bangladesh, maternal VD supplementation did not affect the risk of nasal pneumococcal acquisition, dynamics of carriage or carriage density in the infant offspring up to 6 months of age. As IPD is believed to be caused by recently acquired serotypes in the nasopharynx [8], we reasoned if VD supplementation resulted in a delay in pneumococcal carriage acquisition then supplementation could reduce the risk of IPD during the early postnatal period when host immune function is relatively immature and before infants receive at least two PCV doses. The findings indicate improvements in VD status in early infancy do not delay the age of initial postnatal pneumococcal acquisition. To date, few studies have examined the effect of maternal VD supplementation on infant infectious diseases [33], and no trials specifically examined the effects on pneumococcal carriage or IPD. In the context of accumulated evidence, these findings do not support a role for maternal VD supplementation to reduce the risk of IPD in early infancy through reducing the risk of acquisition or effects on carriage dynamics or density.
Maternal VD supplementation in the MDIG trial improved both maternal and infant 25(OH)D levels at birth with sustained effects in the group of infants born to mothers who received 28,000 IU during the postpartum period [35], such that few infants in the highest-dose group had biochemical VD deficiency up to 6 months of age. However, pneumococcal acquisition rates and carriage dynamics were similar in the high-dose prenatal/postpartum group E compared to placebo, and there was no evidence of a beneficial dose–response effect. Several metrics of carriage dynamics were considered in multi-state modeling, and one difference was the ‘ratio of negative-to-positive: positive-to-negative episodes’ was somewhat higher in group E than the other groups (although with overlapping confidence intervals), findings that would suggest a greater rather than reduced tendency to have a positive carriage state in the high-dose VD group. Pneumococcal density was similar in the high-dose prenatal/postpartum group E compared to placebo, and there was no evidence of a beneficial dose–response effect on density.
The anti-pneumococcal immune response promoted by VD in vitro was characterized by enhanced dendritic cell maturation, reduction of pro-inflammatory cytokines and increased neutrophil-mediated killing [19,20,21]. However, it is possible that these immunomodulating effects of VD are most relevant in the context of a more potent immune stimulus than nasopharyngeal carriage, particularly since innate immune mechanisms may be less important in clearing nasal carriage than in the response to invasive infection [37, 38]. Also, neonatal/infant mouse model studies showed that the clearance of pneumococcal carriage is impaired in neonatal/infant versus adult mice due to reduced macrophage infiltration [39] and lower production of macrophage cytokines involved in neutrophil recruitment and activation [40], suggesting that VD may be more effective in preventing carriage or promoting clearance in older children and adults than in the infants in the present study. However, the deficit in clearing pneumococcal carriage observed in infant mice was ameliorated by immunization [40], and it remains plausible that VD could modify the response to PCV in infants given the known effects of VD on the adaptive immune response [41].
Nearly all infants in the study cohort had pneumococcal acquisition by 6 months of age. Multi-state modeling suggested infants were likely to spend more time in a positive carriage state rather than a negative state, possibly indicating a slower process of clearance of pneumococcus in the nasopharynx compared to the time required to initially acquire pneumococcus or re-acquire it after prior clearance. Cycling between episodes was common throughout the first 6 months of life. In theory, cycling is undesirable if the re-acquisition of pneumococcus results in an increased risk of IPD [9]. However, due to the absence of serotype data in the present study, it was unknown when the infants acquired new serotypes or were recolonized with a serotype acquired in an earlier episode. With increasing age, the probability of being positive for pneumococcal carriage became uncoupled from prior swab status. This observation reinforced the idea that interventions aiming to reduce pneumococcal acquisition in early infancy may not have long-term impacts due to the high overall prevalence of carriage and frequent cycling between positive and negative states. Delaying the age of initial acquisition may not necessarily confer health benefits; acquisition of low-virulence serotypes in early life may reduce the risk of acquisition of pathogenic serotypes due to serotype competition in the nasopharynx through the stimulation of non-serotype specific adaptive immune responses or by limiting the extent to which pathogenic serotypes find an ecological niche for colonization [42,43,44].
The cohort of infants studied had similar carriage rates at 1, 2 and 3 months of age compared to previous studies conducted in Bangladesh [45,46,47]. Pneumococcal carriage dynamics were similar to those observed among infants in Thailand [48], but different from non-serotype specific findings in South Africa and Kenya. In the South Africa cohort, the time to acquisition was longer than the current study, but like the current study, 96% of infants were colonized at least once by 260 days of life [49]. In the Kenyan cohort, the carriage duration was shorter than the current study, but 66% of the children were pneumococcal carriers at least once during the longitudinal study [50].
The study was strengthened by leveraging data from a randomized trial where there was a potent effect of supplementation on VD status in a setting of a high prevalence of maternal-neonatal VD deficiency and where nasal pneumococcal acquisition occurs almost universally in early infancy [45,46,47]. A study limitation was that because swab collection was prompted by ARI criteria, rather than scheduled at specific timepoints, the outcome was conditional on a post-randomization variable. However, we previously showed clinical and virus-associated ARI incidence was unaffected by the VD intervention [33], such that swab collection frequencies were similar across the groups, making bias highly unlikely. Nonetheless, the analyses were based on carriage dynamics during ARI episodes, and it remains possible that our findings would have been different if we had studied carriage during periods in which infants were asymptomatic. As it seemed unlikely that VD supplementation would have a serotype-specific immunomodulatory effect, the resources needed to perform pneumococcal serotyping for the large number of samples were not warranted to address the primary study aims. However, it is plausible that VD could differentially affect serotype acquisition based on its virulence and its propensity to induce an immune response. Serotype data would have enabled a closer examination of carriage dynamics to determine the extent to which negative-to-positive transitions involved newly acquired serotypes.
Conclusion
Maternal VD supplementation did not delay or reduce the rate of pneumococcal carriage or carriage density in early infancy. However, there may be other mechanisms by which VD supplementation enhances the host response to PCV or reduces the risk or severity of IPD. Therefore, given the anti-pneumococcal effects of VD in vitro, further trials designed specifically to examine the effects of VD supplementation on IPD or to enhance the response to vaccination may be warranted in high-risk populations.
Data availability
De-identified individual participant data that underlie the results reported in this article (text, tables, figures, and appendices) and the study protocol will be available immediately after publication and ending 5 years following article publication. These data and documents will be made available to investigators whose secondary data analysis study protocol has been approved by an independent research ethics board. Proposals should be directed to daniel.roth@sickkids.ca; to gain access, data requestors will need to sign a data access agreement.
Abbreviations
- LMICs:
-
Low- and middle-income countries (LMICs)
- IPD:
-
Invasive pneumococcal disease
- PCV:
-
Pneumococcal conjugate vaccine
- PCV10:
-
Ten-valent pneumococcal conjugate vaccine
- LRTI:
-
Lower respiratory tract infections
- VD:
-
Vitamin D
- ARI:
-
Acute respiratory infections
- MDARI:
-
Maternal Vitamin D Supplementation to Prevent Acute Respiratory Infections
- MDIG:
-
Maternal Vitamin D for Infant Growth Trial
- iccdr,b:
-
International Centre for Diarrhoeal Disease Research, Bangladesh
- 25(OH)D:
-
Serum 25-hydroxyvitamin D
- GEE:
-
Generalized estimating equations
References
von Mollendorf C, Tempia S, von Gottberg A, Meiring S, Quan V, Feldman C, et al. Estimated severe pneumococcal disease cases and deaths before and after pneumococcal conjugate vaccine introduction in children younger than 5 years of age in South Africa. PLoS ONE. 2017;12(7):e0179905.
Saha SK, Schrag SJ, El Arifeen S, Mullany LC, Shahidul Islam M, Shang N, et al. Causes and incidence of community-acquired serious infections among young children in south Asia (ANISA): an observational cohort study. Lancet. 2018;392(10142):145–59.
Waters D, Jawad I, Ahmad A, Luksic I, Nair H, Zgaga L, et al. Aetiology of community-acquired neonatal sepsis in low and middle income countries. J Glob Health. 2011;1(2):154–70.
Faust K, Demmert M, Bendiks M, Gopel W, Herting E, Hartel C. Intrapartum colonization with Streptococcus pneumoniae, early-onset sepsis and deficient specific neonatal immune responses. Arch Gynecol Obstet. 2012;285(3):599–604.
Mehr S, Wood N. Streptococcus pneumoniae—a review of carriage, infection, serotype replacement and vaccination. Paediatr Respir Rev. 2012;13(4):258–64.
Faden H, Duffy L, Wasielewski R, Wolf J, Krystofik D, Tung Y. Relationship between nasopharyngeal colonization and the development of otitis media in children. Tonawanda/Williamsville Pediatrics. J Infect Dis. 1997;175(6):1440–5.
Ghaffar F, Friedland IR, McCracken GH Jr. Dynamics of nasopharyngeal colonization by Streptococcus pneumoniae. Pediatr Infect Dis J. 1999;18(7):638–46.
Gray BM, Converse GM 3rd, Dillon HC Jr. Serotypes of Streptococcus pneumoniae causing disease. J Infect Dis. 1979;140(6):979–83.
Gray BM, Converse GM 3rd, Dillon HC Jr. Epidemiologic studies of Streptococcus pneumoniae in infants: acquisition, carriage, and infection during the first 24 months of life. J Infect Dis. 1980;142(6):923–33.
Collins DA, Hoskins A, Snelling T, Senasinghe K, Bowman J, Stemberger NA, et al. Predictors of pneumococcal carriage and the effect of the 13-valent pneumococcal conjugate vaccination in the Western Australian Aboriginal population. Pneumonia (Nathan). 2017;9:14.
Huang SS, Hinrichsen VL, Stevenson AE, Rifas-Shiman SL, Kleinman K, Pelton SI, et al. Continued impact of pneumococcal conjugate vaccine on carriage in young children. Pediatrics. 2009;124(1):e1-11.
Sigurdsson S, Erlendsdottir H, Quirk SJ, Kristjansson J, Hauksson K, Andresdottir BDI, et al. Pneumococcal vaccination: direct and herd effect on carriage of vaccine types and antibiotic resistance in Icelandic children. Vaccine. 2017;35(39):5242–8.
Auranen K, Rinta-Kokko H, Goldblatt D, Nohynek H, O’Brien KL, Satzke C, et al. Design questions for Streptococcus pneumoniae vaccine trials with a colonisation endpoint. Vaccine. 2013;32(1):159–64.
Vu HT, Yoshida LM, Suzuki M, Nguyen HA, Nguyen CD, Nguyen AT, et al. Association between nasopharyngeal load of Streptococcus pneumoniae, viral coinfection, and radiologically confirmed pneumonia in Vietnamese children. Pediatr Infect Dis J. 2011;30(1):11–8.
Short KR, Reading PC, Wang N, Diavatopoulos DA, Wijburg OL. Increased nasopharyngeal bacterial titers and local inflammation facilitate transmission of Streptococcus pneumoniae. mBio. 2012. https://doi.org/10.1128/mBio.00255-12.
Andrews NJ, Waight PA, Burbidge P, Pearce E, Roalfe L, Zancolli M, et al. Serotype-specific effectiveness and correlates of protection for the 13-valent pneumococcal conjugate vaccine: a postlicensure indirect cohort study. Lancet Infect Dis. 2014;14(9):839–46.
Goldblatt D, Southern J, Andrews NJ, Burbidge P, Partington J, Roalfe L, et al. Pneumococcal conjugate vaccine 13 delivered as one primary and one booster dose (1 + 1) compared with two primary doses and a booster (2 + 1) in UK infants: a multicentre, parallel group randomised controlled trial. Lancet Infect Dis. 2018;18(2):171–9.
Madhi SA, Mutsaerts EA, Izu A, Boyce W, Bhikha S, Ikulinda BT, et al. Immunogenicity of a single-dose compared with a two-dose primary series followed by a booster dose of ten-valent or 13-valent pneumococcal conjugate vaccine in South African children: an open-label, randomised, non-inferiority trial. Lancet Infect Dis. 2020;20(12):1426–36.
Hoe E, Nathanielsz J, Toh ZQ, Spry L, Marimla R, Balloch A, et al. Anti-inflammatory effects of vitamin D on human immune cells in the context of bacterial infection. Nutrients. 2016;8(12):806.
Olliver M, Spelmink L, Hiew J, Meyer-Hoffert U, Henriques-Normark B, Bergman P. Immunomodulatory effects of vitamin D on innate and adaptive immune responses to Streptococcus pneumoniae. J Infect Dis. 2013;208(9):1474–81.
Subramanian K, Bergman P, Henriques-Normark B. Vitamin D promotes pneumococcal killing and modulates inflammatory responses in primary human neutrophils. J Innate Immun. 2017;9(4):375–86.
Akhtar E, Mily A, Haq A, Al-Mahmud A, El-Arifeen S, Hel Baqui A, et al. Prenatal high-dose vitamin D3 supplementation has balanced effects on cord blood Th1 and Th2 responses. Nutr J. 2016;15(1):75.
Hornsby E, Pfeffer PE, Laranjo N, Cruikshank W, Tuzova M, Litonjua AA, et al. Vitamin D supplementation during pregnancy: effect on the neonatal immune system in a randomized controlled trial. J Allergy Clin Immunol. 2018;141(1):269–78 e1.
Raqib R, Ly A, Akhtar E, Mily A, Perumal N, Al-Mahmud A, et al. Prenatal vitamin D(3) supplementation suppresses LL-37 peptide expression in ex vivo activated neonatal macrophages but not their killing capacity. Br J Nutr. 2014;112(6):908–15.
Rochat MK, Ege MJ, Plabst D, Steinle J, Bitter S, Braun-Fahrlander C, et al. Maternal vitamin D intake during pregnancy increases gene expression of ILT3 and ILT4 in cord blood. Clin Exp Allergy. 2010;40(5):786–94.
Cebey-Lopez M, Pardo-Seco J, Gomez-Carballa A, Martinon-Torres N, Rivero-Calle I, Justicia A, et al. Role of vitamin D in hospitalized children with lower tract acute respiratory infections. J Pediatr Gastroenterol Nutr. 2016;62(3):479–85.
Chowdhury R, Taneja S, Bhandari N, Sinha B, Upadhyay RP, Bhan MK, et al. Vitamin-D deficiency predicts infections in young north Indian children: a secondary data analysis. PLoS ONE. 2017;12(3):e0170509.
Haugen J, Basnet S, Hardang IM, Sharma A, Mathisen M, Shrestha P, et al. Vitamin D status is associated with treatment failure and duration of illness in Nepalese children with severe pneumonia. Pediatr Res. 2017;82(6):986–93.
Roth DE, Shah MR, Black RE, Baqui AH. Vitamin D status of infants in northeastern rural Bangladesh: preliminary observations and a review of potential determinants. J Health Popul Nutr. 2010;28(5):458–69.
Das RR, Singh M, Naik SS. Vitamin D as an adjunct to antibiotics for the treatment of acute childhood pneumonia. Cochrane Database Syst Rev. 2018;7:CD011597.
Manaseki-Holland S, Maroof Z, Bruce J, Mughal MZ, Masher MI, Bhutta ZA, et al. Effect on the incidence of pneumonia of vitamin D supplementation by quarterly bolus dose to infants in Kabul: a randomised controlled superiority trial. Lancet. 2012;379(9824):1419–27.
Martineau AR, Jolliffe DA, Hooper RL, Greenberg L, Aloia JF, Bergman P, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583.
Morris SK, Pell LG, Rahman MZ, Mahmud AA, Shi J, Ahmed T, et al. Effects of maternal vitamin D supplementation during pregnancy and lactation on infant acute respiratory infections: follow-up of a randomized trial in Bangladesh. J Pediatric Infect Dis Soc. 2021. https://doi.org/10.1093/jpids/piab032.
Jaiswal N, Singh M, Thumburu KK, Bharti B, Agarwal A, Kumar A, et al. Burden of invasive pneumococcal disease in children aged 1 month to 12 years living in South Asia: a systematic review. PLoS ONE. 2014;9(5):e96282.
Roth DE, Morris SK, Zlotkin S, Gernand AD, Ahmed T, Shanta SS, et al. Vitamin D supplementation in pregnancy and lactation and infant growth. N Engl J Med. 2018;379(6):535–46.
Morris SK, Pell LG, Rahman MZ, Dimitris MC, Mahmud A, Islam MM, et al. Maternal vitamin D supplementation during pregnancy and lactation to prevent acute respiratory infections in infancy in Dhaka, Bangladesh (MDARI trial): protocol for a prospective cohort study nested within a randomized controlled trial. BMC Pregnancy Childbirth. 2016;16(1):309.
Calbo E, Garau J. Of mice and men: innate immunity in pneumococcal pneumonia. Int J Antimicrob Agents. 2010;35(2):107–13.
Weiser JN, Ferreira DM, Paton JC. Streptococcus pneumoniae: transmission, colonization and invasion. Nat Rev Microbiol. 2018;16(6):355–67.
Siegel SJ, Tamashiro E, Weiser JN. Clearance of pneumococcal colonization in infants is delayed through altered macrophage trafficking. PLoS Pathog. 2015;11(6):e1005004.
Bogaert D, Weinberger D, Thompson C, Lipsitch M, Malley R. Impaired innate and adaptive immunity to Streptococcus pneumoniae and its effect on colonization in an infant mouse model. Infect Immun. 2009;77(4):1613–22.
Wei R, Christakos S. Mechanisms underlying the regulation of innate and adaptive immunity by vitamin D. Nutrients. 2015;7(10):8251–60.
Masala GL, Lipsitch M, Bottomley C, Flasche S. Exploring the role of competition induced by non-vaccine serotypes for herd protection following pneumococcal vaccination. J R Soc Interface. 2017;14(136):20170620.
Mehtala J, Antonio M, Kaltoft MS, O’Brien KL, Auranen K. Competition between Streptococcus pneumoniae strains: implications for vaccine-induced replacement in colonization and disease. Epidemiology. 2013;24(4):522–9.
Flasche S, Edmunds WJ, Miller E, Goldblatt D, Robertson C, Choi YH. The impact of specific and non-specific immunity on the ecology of Streptococcus pneumoniae and the implications for vaccination. Proc Biol Sci. 2013;280(1771):20131939.
Coles CL, Labrique A, Saha SK, Ali H, Al-Emran H, Rashid M, et al. Newborn vitamin A supplementation does not affect nasopharyngeal carriage of Streptococcus pneumoniae in Bangladeshi infants at age 3 months. J Nutr. 2011;141(10):1907–11.
Granat SM, Mia Z, Ollgren J, Herva E, Das M, Piirainen L, et al. Longitudinal study on pneumococcal carriage during the first year of life in Bangladesh. Pediatr Infect Dis J. 2007;26(4):319–24.
Saha SK, Baqui AH, Darmstadt GL, Ruhulamin M, Hanif M, El Arifeen S, et al. Comparison of antibiotic resistance and serotype composition of carriage and invasive pneumococci among Bangladeshi children: implications for treatment policy and vaccine formulation. J Clin Microbiol. 2003;41(12):5582–7.
Murad C, Dunne EM, Sudigdoadi S, Fadlyana E, Tarigan R, Pell CL, et al. Pneumococcal carriage, density, and co-colonization dynamics: a longitudinal study in Indonesian infants. Int J Infect Dis. 2019;86:73–81.
Dube FS, Ramjith J, Gardner-Lubbe S, Nduru P, Robberts FJL, Wolter N, et al. Longitudinal characterization of nasopharyngeal colonization with Streptococcus pneumoniae in a South African birth cohort post 13-valent pneumococcal conjugate vaccine implementation. Sci Rep. 2018;8(1):12497.
Abdullahi O, Karani A, Tigoi CC, Mugo D, Kungu S, Wanjiru E, et al. Rates of acquisition and clearance of pneumococcal serotypes in the nasopharynges of children in Kilifi District. Kenya J Infect Dis. 2012;206(7):1020–9.
Acknowledgements
We thank the trial participants and their families; the staff of the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Maternal and Child Health Training Institute and Shimantik for their collaboration; Ministry of Health and Family Welfare of Bangladesh for its approval to conduct the trial; present and former staff at the Centre for Global Child Health at The Hospital for Sick Children (Toronto); and the staff at the Bill and Melinda Gates Foundation.
Previous presentation: Taghivand M, Ohuma EO, Pullenayegum EM, Pell LG, Morris SK, Rahman MZ, Mahmud AA, Ahmed T, Hamer DH, Zlotkin SH, Roth DE. Effect of Maternal Vitamin D Supplementation During Pregnancy and Lactation on Early Infant Nasal Pneumococcal Carriage in Bangladesh (P10-125-19). Poster presented at American Society for Nutrition 2019, Baltimore. June 8–11, 2019.
Funding
This work was supported by the Bill and Melinda Gates Foundation (Grant Number OPP1066764). The funders of the study had no role in study design, data collection, analysis, interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
SKM and DER conceived the study and led the protocol design. MT wrote the first draft of the manuscript. AAM and MZR lead the protocol implementation and laboratory analyses, respectively, in Bangladesh. MT, LGP, EOO, TA, JBG, EMP, DHH, and SHZ contributed to study design, analysis, and/or implementation. SKM and DER had full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The MDARI study, including pneumococcal carriage detection protocols, was approved by research ethics committees at the Hospital for Sick Children in Toronto (REB 100039072) and the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) (ERC protocol PR-14079). Written informed consent was obtained from all women for participation in the MDIG and MDARI studies, including consent for storage and use of biological specimens.
Consent for publication
Not applicable.
Competing interests
All authors: No reported conflicts. All authors have submitted the ICMJE Form for Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
MDARI definitions for acute respiratory infections.
Additional file 2: Table S2.
Effect of maternal vitamin D supplementation on risk of pneumococcal acquisition in infants in Bangladesh using an interval-censored model with a day 7 start.
Additional file 3: Table S3.
Effects of maternal vitamin D supplementation of varying doses on the risk of pneumococcal acquisition using a Cox proportional hazard model with day 0 start.
Additional file 4: Table S4.
Effects of maternal vitamin D supplementation of varying doses on the risk of pneumococcal acquisition using a Cox proportional hazard model with day 7 start.
Additional file 5: Table S5.
Effects of maternal vitamin D supplementation of varying doses on infant nasal pneumococcal carriage dynamics using a multi-state model with day 7 start.
Additional file 6: Method S1.
Determination of intervals used in interval-censored model.
Additional file 7: Figure S1.
Probability of change to positive state from a negative state start aggregated across all treatment groups over trial period based on predicted multi-state model probabilities from day 0 to day 189 (N = 3792 swabs).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Taghivand, M., Pell, L.G., Rahman, M.Z. et al. Effect of maternal vitamin D supplementation on nasal pneumococcal acquisition, carriage dynamics and carriage density in infants in Dhaka, Bangladesh. BMC Infect Dis 22, 52 (2022). https://doi.org/10.1186/s12879-022-07032-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07032-y