
Abstract
Introduction
Despite numerous observational studies reporting a positive correlation between polyunsaturated fatty acids (PUFAs) and the risk of sepsis and mortality, the causation of such an association has yet to be firmly established. Thus, our study aimed to undertake the Mendelian randomization (MR) approach to scrutinize the potential causalities of PUFAs with sepsis and mortality risk.
Methods
We conducted the MR investigation using genome-wide association study (GWAS) summary statistics of PUFAs [including omega-3 fatty acids (omega-3), omega-6 fatty acids (omega-6), the ratio of omega-6 to omega-3 fatty acids (omega-6:3), docosahexaenoic acid (DHA), linoleic acid (LA)], sepsis, and sepsis mortality. We utilized the GWAS summary data from the UK Biobank. To establish reliable causality, we employed the inverse-variance weighted (IVW) method as the primary analytical approach, together with four additional MR methods. In addition, we performed heterogeneity and horizontal pleiotropy assessments using Cochrane’s Q test and MR-Egger intercept test, respectively. Finally, we performed a series of sensitivity analyses to enhance the precision and veracity of our findings.
Results
The IVW method showed that genetically predicted omega-3 [odd ratio (OR) 0.914, 95% confidence interval (CI) 0.845–0.987, P = 0.023] and DHA (OR 0.893, 95% CI 0.815–0.979, P = 0.015) were suggestively linked to a decreased risk of sepsis. Furthermore, genetically predicted DHA (OR 0.819, 95% CI 0.681–0.986, P = 0.035) was suggestively associated with a reduced risk of sepsis-related death. Conversely, the omega-6:3 ratio (OR 1.177, 95% CI 1.011–1.371, P = 0.036) was suggestively linked to an increased risk of sepsis-induced mortality. On the basis of the MR-Egger intercept assessment, it appears that our MR examination was not influenced by any horizontal pleiotropy (all P > 0.05). Moreover, the reliability of the estimated causal association was confirmed by the sensitivity analyses.
Conclusion
Our study supported the casual effect between PUFAs and susceptibility to sepsis and sepsis-related death. Our findings underline the importance of specific PUFAs levels, particularly for individuals with a genetic susceptibility to sepsis. Further research is needed to confirm these findings and investigate the underlying mechanisms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Sepsis is a significant threat to global health and patient safety, and identifying potential risk factors for sepsis is crucial in mitigating its incidence and associated mortality rates. |
Although many observational studies have reported a positive correlation between polyunsaturated fatty acids (PUFAs) and sepsis, the causal relationship has not been firmly established. |
Our study aimed to undertake the Mendelian randomization (MR) approach to scrutinize the potential causalities of PUFAs on the risk of sepsis and sepsis-related mortality. |
What was learned from the study? |
This study is the first to examine the causal relationship between PUFAs and the risk of sepsis and mortality using an MR approach. |
Genetically predicted omega-3 and docosahexaenoic acid (DHA) were suggestively associated with a lower risk of sepsis. Moreover, the genetically predicted DHA was also suggestively associated with a decreased risk of sepsis mortality. Conversely, the ratio of omega-6:3 was suggestively associated with a higher risk of sepsis mortality. |
Overall, our findings underscore the significance of PUFAs in evaluating sepsis and mortality risk, which may offer potential opportunities for personalized preventive strategies. |
Introduction
Sepsis, defined as life-threatening organ dysfunction caused by a dysregulated host response to infection, continues to be a formidable cause of morbidity and mortality globally [1]. According to estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), there were approximately 48.9 million new cases of sepsis in 2017, resulting in nearly 11.0 million deaths worldwide [2]. Given sepsis has been recognized as a significant threat to global health and patient safety by the World Health Organization (WHO), identifying potential risk factors for sepsis is crucial in mitigating its incidence and associated mortality rates [3].
Polyunsaturated fatty acids (PUFAs) are essential nutrients that play a crucial role in the development and progression of several infectious diseases. Among them, a heightened level of omega-3 fatty acids and docosahexaenoic acid (DHA) have been demonstrated to be associated with improved sepsis outcomes in both experimental and observational studies [4,5,6,7,8,9]. However, traditional observational studies could not entirely exclude confounding biases or reverse causality. Furthermore, there is insufficient evidence gathered from randomized controlled trials (RCTs) to substantiate their relationships. Hence, the causality between PUFAs and the risk of sepsis and mortality are not well established.
The Mendelian randomization (MR) approach represents a popular methodology for assessing causal inference between exposure and outcome. Notably, MR leverages single nucleotide polymorphisms (SNPs) as instrumental variables (IVs), thereby constituting a quasi-RCT, as the genetic variants are ascribed randomly at the time of conception and are not influenced by confounding factors. Recent research has used the MR technique to probe the causal links between PUFAs and various ailments, such as bone mineral density and fracture [10], kidney function [11], and schizophrenia [12]. Therefore, the aim of this study was to undertake the MR approach to scrutinize the potential causalities between PUFAs and the risk of sepsis and sepsis-related mortality.
Methods
Study Design
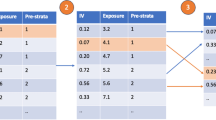
We utilized an MR method, employing summary statistics obtained from genome-wide association studies (GWAS), to investigate the relationship between PUFAs [including omega-3 fatty acids (omega-3), omega-6 fatty acids (omega-6), the ratio of omega-6 to omega-3 fatty acids (omega-6:3), DHA, and linoleic acid (LA)], sepsis, and sepsis mortality at 28 days. To ensure the validity of the MR analysis, we relied upon three core assumptions: (i) the genetic variants used should be significantly associated with the exposure of interest; (ii) the genetic variants employed should not have an impact on the outcome, except through that exposure; and (iii) the genetic variants should not be linked to any confounders affecting the relationship of the exposure to the outcome. The study design is detailed in Fig. 1.

Overall design of the present study. SNP single nucleotide polymorphism
Ethics Statement
The analysis in this article is based on previously publicly available data and does not involve any new studies of human or animal subjects performed by any of the authors. All of the GWAS data sets utilized in this investigation were openly accessible in the general public domain, negating the need for individual ethical approval or informed consent. Furthermore, the findings of this study were presented in strict accordance with the guidelines presented in the Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) guidance in 2021 [13].
Genetic Associations with PUFAs
We examined five primary dietary PUFA indices, namely omega-3, omega-6, the ratio of omega-6:3, DHA, and LA. Our investigation utilized genetic instrumentation to obtain information on omega-3 (N = 114,999), omega-6 (N = 114,999), the ratio of omega-6:3 (N = 114,999), DHA (N = 114,999), and LA (N = 114,999) from the Metabolic Biomarkers in the UK Biobank [14]. The UK Biobank is an initiative aimed at exploring the genetic and environmental contributors to disease, with more than 500,000 individuals of European ancestry included in the recruitment. This project utilized a targeted high-throughput nuclear magnetic resonance (NMR) metabolomics platform (biomarker quantification version 2020) provided by Nightingale Health Ltd to assess the circulating concentrations of omega-3, omega-6, DHA, and LA, in randomly selected EDTA plasma samples. Of the initially collected 121,577 samples, duplicates and observations that did not meet quality control criteria in the non-fasting plasma samples collected at baseline were excluded, leaving a final data set of 114,999 samples. The measurement technology and applications of this platform for epidemiological studies have been previously evaluated [15, 16]. Genetic associations with PUFAs can be found in Table 1.
Genetic Associations with Sepsis and Sepsis Mortality
We obtained genetic association estimations for SNPs linked to sepsis [IEU GWAS ID: ieu-b-4980; N = 486,484 (11,643 cases and 474,841 controls)] and sepsis mortality at 28 days [IEU GWAS ID: ieu-b-5086; N = 486,484 (1896 cases and 484,588 controls)] from the GWAS outcomes of the UK Biobank [17, 18]. Specifically, sepsis cases were identified using International Classification of Diseases (ICD) 10th edition codes A02, A39, A40, and A41, which are consistent with the definitions used in recent literature [19]. These estimations were easily accessed via the Integrative Epidemiologic Unit (IEU) GWAS database at https://gwas.mrcieu.ac.uk/. Table 1 provides the details of the genetic associations with sepsis and sepsis-related mortality.
Instrumental Variables Selection
To investigate the causal associations between PUFAs and sepsis risk and mortality, we utilized IVs in our MR analysis. The IVs acted as mediators between exposures and outcomes, and were obtained by searching GWAS data for leading SNPs associated with PUFAs. We set rigorous screening criteria for these IVs. SNPs that demonstrated strong associations with PUFAs at a genome-wide level of significance (P < 5 × 10−8) were selected, and further filtered for a window size greater than 10,000 kb and a linkage disequilibrium level (r2 < 0.001) to minimize any potential effects due to linkage disequilibrium. Palindromic SNPs, outcome-related SNPs (P < 5 × 10−8), and SNPs not present in outcome GWAS summary data were excluded from the IVs. Furthermore, we removed any SNPs with F statistics less than 10 to ensure a strong association between IVs and PUFAs. Our rigorous selection criteria and use of IVs helped to establish robust causal associations between PUFAs and the risk of sepsis and sepsis mortality.
MR Analysis
Five common analytical methods were employed to examine the connection between PUFAs and sepsis risk and mortality, namely random-effects inverse-variance weighted (IVW), MR-Egger, weighted median, simple mode, and weighted mode. Among these methods, IVW was considered as the primary MR analysis due to its high statistical power, which combines the Wald ratio estimates of each SNP on the outcome to obtain a pooled causal estimate. Additionally, four other MR methods were utilized to further strengthen the findings. The MR-Egger method provided consistent estimations of the causative effect under the instrument strength independent of direct effect assumption [20]. The weighted median method offered solid estimates of effective IVs accounting for more than 50% of the weight [21]. The simple mode approach provided robustness against pleiotropy by utilizing a model-based assessment approach, while the weighted mode method was employed to evaluate the robustness of the IVW method results [22]. As a result, the IVW method findings were defined as the main results of this MR study.
Heterogeneity, Horizontal Pleiotropy and Sensitivity Analysis
Heterogeneity among individual SNP estimates was identified using the Cochran’s Q test, with a P value below 0.05 indicating potential heterogeneity. Nevertheless, the mere presence of heterogeneity does not necessarily invalidate the IVW result. To assess the possibility of horizontal pleiotropy, we applied the MR-Egger intercept test, with a P value below 0.05 indicating a possible pleiotropic effect. We conducted various sensitivity analyses, including scatter plot inspection, leave-one-out analysis, and funnel plot inspection. The scatter plot was utilized to determine the causal relationship between PUFAs and the risk of sepsis and sepsis mortality. The leave-one-out analysis allowed us to assess whether the results were significantly impacted by the removal of a single SNP. Finally, the funnel plot was implemented to evaluate the possibility of horizontal pleiotropy.
Statistical Analyses
The potential for sample overlap between the PUFAs and sepsis populations can introduce confounding relationships in the MR estimates when weak instruments are involved. We then utilized a web calculator to formally evaluate the risk of bias resulting from sample overlap [23], which can be accessed at https://sb452.shinyapps.io/overlap. To adjust for multiple testing in our MR study, we applied a Bonferroni correction with 10 tests, yielding a significance threshold of P < 0.005 (0.05/10). Those that were significant (P < 0.05) before but not after Bonferroni correction (P < 0.005) were considered as the suggestive association results. To estimate the causal effect of PUFAs on the risk of sepsis and sepsis-related mortality, we calculated the odds ratios (ORs) with corresponding 95% confidence intervals (CIs). All statistical analyses were conducted using R software (version 4.2.1) with the “TwoSampleMR” package.
Results
Characteristics of Genetic Variants
After utilizing the genome-wide significance cutoff of 5 × 10−8 for screening, we were able to identify a total of 47 SNPs that were associated with omega-3, 50 SNPs associated with omega-6, 34 SNPs linked to the ratio of omega-6:3, 39 SNPs pertaining to DHA, as well as 43 SNPs relating to LA. After a formal assessment, we found that the risk of bias resulting from sample overlap was small, with a value of less than 3.6%, irrespective of the proportion of overlap. It is worth noting that all F statistic values exceeded 10, indicating a robust relationship between IVs and each PUFAs. Details of these information are presented in Supplementary Tables S1–S5.
MR Analysis: PUFAs as Exposure, Sepsis as Outcome
Table 2 displays the MR analyses regarding to the causal associations of PUFAs with the risk of sepsis. Our IVW method yielded suggestive evidence of a decreased risk of sepsis associated with genetically predicted omega-3 (OR 0.914, 95% CI 0.845–0.987, P = 0.023) and DHA (OR 0.893, 95% CI 0.815–0.979, P = 0.015). However, we found no significant associations between omega-6 (OR 0.920, 95% CI 0.825–1.025, P = 0.131), the ratio of omega-6:3 (OR 1.075, 95% CI 0.993–1.164, P = 0.073), or LA (OR 0.966, 95% CI 0.870–1.072, P = 0.515) and sepsis risk. The findings of MR-Egger, weighted median, simple mode, and weighted mode tallied with those obtained through the IVW approach.
MR Analysis: PUFAs as Exposure, Sepsis Mortality as Outcome
Table 3 depicts the MR analyses on the casual associations between PUFAs and the risk of sepsis mortality at 28 days. The IVW method indicated that genetically predicted DHA was suggestively related to a decreased risk of sepsis mortality (OR 0.819, 95% CI 0.681–0.986, P = 0.035). Nonetheless, the ratio of omega-6:3 was also suggestively linked to an increased risk of sepsis mortality (OR 1.177, 95% CI 1.011–1.371, P = 0.036). Still, no substantial evidence exists to support the genetic causal relationship between omega-3 (OR 0.887, 95% CI 0.755–1.042, P = 0.144), omega-6 (OR 0.973, 95% CI 0.773–1.225, P = 0.815), or LA (OR 1.151, 95% CI 0.913–1.453, P = 0.234) and the risk of sepsis mortality. The findings of MR-Egger, weighted median, simple mode, and weighted mode tallied with those obtained through the IVW approach.
Heterogeneity, Horizontal Pleiotropy, and Sensitivity Analysis
Table 4 presents the findings from Cochrane’sQ test and pleiotropy test. Specifically, our analysis indicated that there was potential heterogeneity in the MR analyses of omega-3 and sepsis (Cochrane’s Q = 75.5, P = 0.004), omega-6 and sepsis (Cochrane’s Q = 79.6, P = 0.004), the ratio of omega-6:3 and sepsis (Cochrane’s Q = 53.2, P = 0.014), DHA and sepsis (Cochrane’s Q = 58.1, P = 0.020), and LA and sepsis (Cochrane’s Q = 58.5, P = 0.046). Nevertheless, the MR-Egger intercept tests suggested that there was no horizontal pleiotropy in any of these analyses, as all P values were above 0.05. Scatter plots for all MR analyses are provided in Supplementary Figs. S1–S2. Our leave-one-out analyses demonstrated that the causal effects of PUFAs on the risk of sepsis and sepsis mortality remained unequivocally robust (Supplementary Figs. S3–S4). Furthermore, the funnel plots for all MR analyses revealed that horizontal pleiotropy was not apparent, as the variation in effect size around the point estimate was symmetrical (Supplementary Figs. S5–S6).
Discussion
This MR study utilized large-scale GWAS summary data to investigate the causal relationship between PUFAs and the risk of sepsis and sepsis mortality in individuals of European ancestry. The results suggested that genetically predicted omega-3 and DHA were suggestively associated with a lower risk of sepsis. Moreover, we demonstrated that genetically predicted DHA was also suggestively related to a decreased risk of sepsis mortality. Conversely, the ratio of omega-6:3 was suggestively associated with a higher risk of sepsis mortality. To our knowledge, this study is the first to examine the causal relationship between PUFAs and sepsis risk and mortality using an MR approach. Overall, our findings underscore the significance of PUFAs in evaluating sepsis and mortality risk, which may offer potential opportunities for personalized preventive strategies.
Our results were in line with a recent meta-analysis of omega-3 therapy, which encompassed 17 RCTs with 1239 patients with sepsis. The investigators reported that compared with no supplementation or placebo, omega-3 supplementation did not significantly impact sepsis mortality risk (RR 0.85, 95% CI 0.71–1.03, P = 0.10) [24]. Nevertheless, our study had uncovered a novel causal association between omega-3 intake and lower sepsis risk, which has not been reported by either observational or randomized studies. DHA is another crucial PUFA component. A prior RCT examining the effect of DHA supplementation on neonates with sepsis showed that DHA administration boosted total body mass and body fat mass significantly, compared to placebo [25]. Consistent with the aforementioned evidence, our findings also indicated that DHA intake is correlated with decreased sepsis risk and mortality associated with sepsis. Previous investigations predominantly focused on total PUFA levels or omega-3 levels alone, disregarding vital interplay between omega-3 and omega-6 levels as a result of the difficulty in clarifying the effect of omega-6:3 ratios on sepsis mortality risk due to confounding factors. We observed that the omega-6:3 ratio is associated with a higher risk of sepsis mortality, partially in agreement with Kaliannan et al.’s findings that a lower omega-6:3 ratio can lead to favorable changes in chronic diseases and cancer [26].
Although the precise causal mechanisms underlying the effects of PUFAs on sepsis risk and mortality remain incompletely understood, several explanations have been posited by researchers. With respect to omega-3, one potential mechanism involves the ability of these fatty acids to mitigate organ damage induced by sepsis by means of downregulating miR-1-3p, elevating Notch3 expression, and obstructing Smad pathway activation [4]. Other possible explanations include anti-inflammatory and antithrombotic effects [27]. For DHA, animal experiments have demonstrated that DHA supplementation can significantly reduce septic shock-induced vascular inflammation, oxidative stress, and production of nitric oxide, all of which serve to improve outcomes [8]. As for the omega-6:3 ratio, previous research suggested that an increased ratio can lead to elevated intestinal permeability, metabolic endotoxemia, and chronic low-grade inflammation, highlighting the importance of limiting omega-6 intake while increasing omega-3 intake to enhance health [26]. Taken together, maintaining sufficient PUFA intake through dietary balance or supplementation represents a crucial strategy for reducing the risk of sepsis and sepsis-related mortality.
The findings of this study can have important clinical implications. We found that maintaining appropriate levels of PUFAs, particularly omega-3 and DHA, may be beneficial in reducing the risk of sepsis. Therefore, healthcare professionals may consider recommending increased intake of foods rich in PUFAs or supplements for individuals at high risk of sepsis, particularly those with a genetic susceptibility. However, it is important to note that the study’s findings are based on a genetic analysis and further research is needed to confirm the clinical usefulness of these recommendations.
This MR study has the following strengths. First, it used a genetic variant as an IV to infer causality between the PUFAs and the risk of sepsis and mortality. The MR approach minimizes the potential for confounding and reverse causation, which are major concerns in traditional observational studies [28,29,30]. Second, this study used large-scale genomic data from the UK Biobank, increasing the generalizability and robustness of the findings. Third, the use of publicly available data sets and open source software enhanced the transparency and reproducibility of the study. Fourth, the approach allows for estimation of the causal effect size, which could have important implications for clinical and public health decision-making. Overall, this MR study provided important insights into the causal relationship between the PUFAs and the risk of sepsis and mortality, and highlights the importance of addressing modifiable risk factors for improving health outcomes.
Despite its advantages, our study also has several limitations that must be acknowledged. First, the reliance on data from GWAS that exclusively included individuals of European ancestry precludes the generalization of our findings to other ethnic groups, which limits the study’s cultural diversity dimension. Yet, it is worth noting that the homogeneity of the sample reduces the risk of confounding by population admixture. Second, there was partial sample overlap between the PUFAs and sepsis. However, the relative bias from sample overlap is also very small (< 3.6%), which might not interfere with our overall conclusion. Third, our study lacked appropriate sensitivity analyses to evaluate the possibility of horizontal pleiotropy, despite conducting the MR-Egger intercept test and finding that horizontal pleiotropy was not apparent in our statistical analyses. Fourth, we observed heterogeneity in some of our results. Nonetheless, the random-effect IVW remained the principal analytical method, which effectively controls the pooled heterogeneity of the data. Fifth, we exclusively rely on genetic-level evidence, which precludes further observation studies and mediator analyses to validate the particular regulatory mechanisms that operate in the causality between PUFAs and susceptibility to sepsis and sepsis-related mortality. Therefore, future studies need to be conducted on larger and more diverse populations with different ancestries and cultures, and should employ a combination of observational and genetic techniques to further explore the causal effects of PUFAs on the risk of sepsis and mortality.
Conclusion
Our study supported the casual effect between PUFAs and susceptibility to sepsis and sepsis-related death. Our findings underline the importance of specific PUFAs levels, particularly for individuals with a genetic susceptibility to sepsis. Further research is needed to confirm these findings and investigate the underlying mechanisms.
References
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–10.
Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–11.
Reinhart K, Daniels R, Kissoon N, et al. Recognizing sepsis as a global health priority—a WHO resolution. N Engl J Med. 2017;377(5):414–7.
Chen YL, Xie YJ, Liu ZM, et al. Omega-3 fatty acids impair miR-1-3p-dependent Notch3 down-regulation and alleviate sepsis-induced intestinal injury. Mol Med. 2022;28(1):9.
Liu P, Li M, Wu W, et al. Protective effect of omega-3 polyunsaturated fatty acids on sepsis via the AMPK/mTOR pathway. Pharm Biol. 2023;61(1):306–15.
Korner A, Schlegel M, Theurer J, et al. Resolution of inflammation and sepsis survival are improved by dietary omega-3 fatty acids. Cell Death Differ. 2018;25(2):421–31.
Wolbrink DRJ, Grundsell JR, Witteman B, et al. Are omega-3 fatty acids safe and effective in acute pancreatitis or sepsis? A systematic review and meta-analysis. Clin Nutr. 2020;39(9):2686–94.
Boivin A, Burban M, Clere-Jehl R, et al. Docosahexaenoic acid, but not eicosapentaenoic acid, improves septic shock-induced arterial dysfunction in rats. PLoS ONE. 2017;12(12): e0189658.
Das UN. Combination of aspirin with essential fatty acids is superior to aspirin alone to prevent or ameliorate sepsis or ARDS. Lipids Health Dis. 2016;15(1):206.
Tao SS, Wang P, Wang XY, et al. Causal effect of polyunsaturated fatty acids on bone mineral density and fracture. Front Nutr. 2022;9:1014847.
Huang Y, Wang J, Yang H, et al. Causal associations between polyunsaturated fatty acids and kidney function: a bidirectional Mendelian randomization study. Am J Clin Nutr. 2023;117(1):199–206.
Gao Y, Hu X, Wang D, et al. Association between arachidonic acid and the risk of schizophrenia: a cross-national study and Mendelian randomization analysis. Nutrients. 2023;15(5):1195.
Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–21.
Shin SY, Fauman EB, Petersen AK, et al. An atlas of genetic influences on human blood metabolites. Nat Genet. 2014;46(6):543–50.
Li Y, Li Q, Cao Z, et al. The causal association of polyunsaturated fatty acids with allergic disease: a two-sample Mendelian randomization study. Front Nutr. 2022;9: 962787.
Julkunen H, Cichonska A, Slagboom PE, et al. Metabolic biomarker profiling for identification of susceptibility to severe pneumonia and COVID-19 in the general population. Elife. 2021. https://doi.org/10.7554/eLife.63033.
Hamilton F, Mitchell R, Ahmed H, et al. An observational and Mendelian randomisation study on iron status and sepsis. Sci Rep. 2023;13(1):2867.
Hamilton FW, Thomas M, Arnold D, et al. Therapeutic potential of IL6R blockade for the treatment of sepsis and sepsis-related death: a Mendelian randomisation study. PLoS Med. 2023;20(1): e1004174.
Zekavat SM, Lin SH, Bick AG, et al. Hematopoietic mosaic chromosomal alterations increase the risk for diverse types of infection. Nat Med. 2021;27(6):1012–24.
Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–25.
Bowden J, Davey Smith G, Haycock PC, et al. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–14.
Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–98.
Burgess S, Davies NM, Thompson SG. Bias due to participant overlap in two-sample Mendelian randomization. Genet Epidemiol. 2016;40(7):597–608.
Lu C, Sharma S, McIntyre L, et al. Omega-3 supplementation in patients with sepsis: a systematic review and meta-analysis of randomized trials. Ann Intensive Care. 2017;7(1):58.
Lopez-Alarcon M, Bernabe-Garcia M, Del Prado M, et al. Docosahexaenoic acid administered in the acute phase protects the nutritional status of septic neonates. Nutrition. 2006;22(7–8):731–7.
Kaliannan K, Li XY, Wang B, et al. Multi-omic analysis in transgenic mice implicates omega-6/omega-3 fatty acid imbalance as a risk factor for chronic disease. Commun Biol. 2019;2:276.
Makris GC, Geroulakos G, Makris MC, et al. The pleiotropic effects of statins and omega-3 fatty acids against sepsis: a new perspective. Expert Opin Investig Drugs. 2010;19(7):809–14.
Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–96.
Mukamal KJ, Stampfer MJ, Rimm EB. Genetic instrumental variable analysis: time to call Mendelian randomization what it is. The example of alcohol and cardiovascular disease. Eur J Epidemiol. 2020;35(2):93–7.
Ference BA. Mendelian randomization studies: using naturally randomized genetic data to fill evidence gaps. Curr Opin Lipidol. 2015;26(6):566–71.
Acknowledgements
Funding
No funding was received for this study. The journal’s Rapid Service fee was supported by the authors.
Author Contributions
Conception and design: Peipei Lei, Weiwei Xu. Administrative support: Songmei Yu, Yanli Guo. Acquisition of data: Peipei Lei, Weiwei Xu. Data analysis and interpretation: Peipei Lei, Congjie Wang, Guoshuai Lin. Manuscript writing: Peipei Lei, Weiwei Xu. Critical revision of the manuscript for important intellectual content: Songmei Yu, Yanli Guo. All authors read and approved the final version of the article, including the authorship list.
Disclosures
All the authors, including Peipei Lei, Weiwei Xu, Congjie Wang, Guoshuai Lin, Songmei Yu and Yanli Guo, have nothing to disclose.
Compliance with Ethics Guidelines
The analysis in this article is based on previously publicly available data and does not involve any new studies of human or animal subjects performed by any of the authors. All of the GWAS data sets utilized in this investigation were openly accessible in the general public domain, negating the need for individual ethical approval or informed consent. Furthermore, the findings of this study were presented in strict accordance with the guidelines presented in the Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) guidance in 2021 [13].
Data Availability
The PUFAs summary data are available in UK Biobank. Sepsis and sepsis mortality summary data are available at https://gwas.mrcieu.ac.uk/.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lei, P., Xu, W., Wang, C. et al. Mendelian Randomization Analysis Reveals Causal Associations of Polyunsaturated Fatty Acids with Sepsis and Mortality Risk. Infect Dis Ther 12, 1797–1808 (2023). https://doi.org/10.1007/s40121-023-00831-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-023-00831-z