
Abstract
Violence is a public health issue that disproportionately affects communities of color in urban centers. There is limited understanding of how violent crime is associated with adult physical inactivity and obesity prevalence given the racial/ethnic composition of community residents. This research aimed to address this gap by examining census tract-level data in Chicago, IL. Ecological data gathered from a variety of sources were analyzed in 2020. Violent crime rate represented the number of police-reported incidents of homicide, aggravated assault, and armed robbery per 1,000 residents. Spatial error and ordinary least square regression models were evaluated to determine if violent crime rate was significant associated with prevalence (%) of adult physical inactivity and obesity among all Chicago census tracts (N = 798), majority non-Hispanic (NH) White tracts (n = 240), majority NH Black tracts (n = 280), majority Hispanic tracts (n = 169), and racially diverse tracts (n = 109). Majority was defined as ≥ 50% representation. After adjusting for socioeconomic and environmental measures (e.g., median income, grocery store availability, walkability index), violent crime rate was associated with % physical inactivity and % obesity at the census tract level in Chicago, IL (both p < 0.001). Associations were statistically significant among majority NH Black and Hispanic tracts, but not majority NH White and racially diverse tracts. Future studies should evaluate the structural drivers of violence and the influence these drivers have on adult physical inactivity and obesity risk, particularly in communities of color.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Violent crime (e.g., homicide, armed robbery, aggravated assault) is widely considered a public health concern in the USA [1, 2]. While the country’s violent crime rate has declined significantly since the 1990s, small upticks have been reported since 2015 [3, 4]. Furthermore, violent crime rates spiked in several US cities in the latter months of 2020 due to the COVID-19 pandemic [5]. Large urban cities, such as Chicago, IL, continue to have disproportionately high violent crime rates [6]. In 2019, the Chicago Department of Public Health reported that the city’s crime rate declined by 16.8% from 2010 to 2018; however, the rate of some major violent crimes, such as homicide, increased during that period [6].
Violent crime rates in Chicago are not comparable across the city’s community areas. Historically, rates have been higher in communities on the city’s south and west sides, which have more minority residents and higher poverty rates [6]. State surveillance data indicate that Chicago’s majority non-Hispanic (NH) Black and Hispanic communities have higher firearm-related homicide rates than majority NH White communities [7]. Furthermore, NH Black adults in Chicago are significantly more likely to report exposure to community violence than NH White adults [8, 9]. These findings highlight the issue of violent crime in Chicago and its disproportionate effects on the Chicago’s communities of color.
Violent crime is a social determinant of health and a manifestation of structural inequities that exist in urban cities [10, 11]. Crime is often worst in communities with limited resources (i.e., job and educational opportunities) and poor physical infrastructure (i.e., built environment) [11]. For example, prior studies have linked crime rates to integral socioeconomic and structural factors including housing value, blight, availability of liquor retailers, and availability of green space [12,13,14]. Given the historical connections between racial/ethnic community composition and structural inequities in resource availability and built environment [15], it is important to strengthen the field’s understanding of the relationship between community violence and community health.
For decades, researchers have studied the harmful effects of violent crime on human health and well-being at the individual and community levels [1, 10]. Two outcomes studied often in this space are physical inactivity and obesity, both strong predictors of chronic disease development (e.g., hypertension, type 2 diabetes, and cardiovascular disease) [16]. Overall, studies have reported that increased levels of violent crime in a community are associated with decreased levels of physical activity among adults and children [17,18,19,20,21,22]. Crime influences perceptions of community safety, which deters community residents from being engaging in outdoor leisurely activities [17,18,19]. Because physical inactivity is highly correlated with obesity, several studies have linked violent crime to obesity as well [23,24,25,26,27,28].
Despite the large body of evidence connecting violent crime to physical inactivity and obesity, no study has examined associations given the racial/ethnic composition of community residents. Thus, the objective of this study was to (1) examine census tract-level associations between violent crime rate, adult physical inactivity, and adult obesity in Chicago, IL, after controlling for key socioeconomic and environmental factors (e.g., median income, walkability, availability of park space) and (2) identify differences in associations by racial/ethnic composition of residents. This information is needed to provide additional context to the significance of community violence in shaping adult health and health behavior. Furthermore, this research can provide more insight to violence as a manifestation of structural inequities in historically disadvantaged communities of color in large urban centers. We hypothesized that violent crime rate is significantly associated with the prevalence of physical inactivity and obesity in Chicago after controlling for relevant sociodemographic and environmental factors. Furthermore, we hypothesize that the strength of associations will vary by the racial/ethnic composition of residents.
Materials and Methods
Data Sources and Measures
Violent Crime
To address our research aims, we conducted an ecological assessment of census tract-level spatial data representative of Chicago, IL, in 2020. There are 801 census tracts within Chicago’s city limits; however, 3 tracts were nonresidential. Thus, our analytical sample comprised 798 census tracts. Our independent variable of interest for this research was violent crime rate, which we estimated for each census tract using 2018 data obtained from the Chicago Citizen Law Enforcement and Reporting (CLEAR) database [29]. CLEAR provides exact XY coordinates for police reported incidents of violent crimes in the City of Chicago [29]. For this study, we aggregated the point data for crime at the census tract level. Our definition of violent crime includes homicide, armed robbery, and aggravated assault; the Federal Bureau of Investigation considers all three offenses a violent crime [30]. We adjusted the total number of crime events by the tract’s population size. Thus, we defined violent crime rate as the number of violent crimes reported to the police in 2018 per 1,000 census tract residents.
Physical Inactivity and Obesity
Our two dependent variables were prevalence (i.e., %) of physical inactivity and obesity among adults (age ≥ 18 years). Data for both measures reflect 2017 estimates produced by the Centers for Disease Control and Prevention (CDC) PLACES project [31]. The CDC’s PLACES project provides census tract-level estimates for 27 measures related to unhealthy behavior, health outcomes, and use of preventive services for 500 of the largest US cities; additional details are available online [31]. Percent physical inactivity represents the percentage of adult citizens who (1) do not meet CDC recommendations for physical activity or (2) report having no leisure time for physical activity. The CDC recommends that adults ages 18–64 engage in at least 150 minutes of moderate intensity activity per week along with strength training [32]. Percent obesity reflects the percentage of adult citizens residing in the census tract who are obese according to their body mass index (BMI). BMI is a measure of adiposity that is calculated by dividing a person’s weight in kilograms by their height in meters squared. A BMI of 30.0 (or higher) is considered obese [33].
Community Racial/Ethnic Composition
To evaluate the role of racial/ethnic composition of community residents, we obtained census tract-level data on the following indicators from the US Census Bureau: % NH White, % NH Black, % Hispanic, and % Asian [34]. With these data, we created variables representing majority White census tracts, majority Black census tracts, majority Hispanic census tracts, and racially diverse census tracts. “Majority” was defined as ≥ 50% representation among tract residents. Census tracts that did not have ≥ 50% representation from NH White, NH Black, or Hispanic residents were labeled “racially diverse.” We identified 4 census tracts where majority of residents were NH Asian. Given the small number of majority NH Asian tracts, these tracts were included in the racially diverse category. Overall, 240 (30.1%), 280 (35.1%), 169 (21.2%), and 109 (13.7%) census tracts were labeled majority NH White, NH Black, Hispanic, and racially diverse, respectively. All race/ethnicity measures reflect 2018 estimates from the US Census Bureau [33].
Covariates
We gathered census tract-level data representing median household income and various environmental amenities (i.e., grocery store availability, % park space, and walkability) to control for these factors in our analyses. We categorized census tracts according to their median household income to identify higher income vs. lower income census tracts. Lower-income census tracts had a median income < $55,295, which was the city median in 2018 according to the U.S. Census [34]. We used the Chicago Grocery Store dataset (retrieved from the Chicago Data Portal) to calculate the number of grocery stores in each tract [35]. This dataset provides location data for all large and chain grocery stores within the city. We defined grocery store availability as the number of stores per 1,000 tract residents in 2018. We used the Park District Boundaries dataset (retrieved from the Chicago Data Portal) to calculate % park space [36]. This measure represents the percentage of the census tract’s land mass that is a city designated park or green space and reflects the 2016 estimate. We retrieved 2017 data on walkability from the United States Environmental Protection Agency (EPA) [37]. The National Walkability Index is a nationwide geographic data resource that ranks block groups according to their relative walkability. The index ranges from numbers 1 to 20. A higher score out of 20 represents a more walkable geographic area.
Statistical Analysis
We used ArcGIS Pro 2.6.1 to create bivariate maps that display the spatial distribution of violent crime rates among census tracts relative to the prevalence of physical inactivity and obesity. Bivariate maps capture the relationship between two variables in one map based on the empirical distribution of values within the dataset [38]. We used ArcGIS 10.7.1 and GeoDa software to analyze the data. We calculated descriptive statistics (i.e., median and range) for our measures of interest among all census tracts in Chicago, IL, and stratified by racial/ethnic composition of residents. We ran Kruskal–Wallis tests to determine if descriptive statistics varied significantly across the four groups representing community racial/ethnic composition: majority NH White, majority NH Black, majority Hispanic, and racially diverse.
To determine if violent crime rate is significantly associated with % physical inactivity and % obesity among all Chicago census tracts, we ran spatial error models. This model allowed us to account for the spatial dependency of census tracts. We reported lambda (λ), the spatial autoregressive coefficient, to indicate the significance of the spatial dependency; a p value < 0.05 for the λ estimate suggests significant spatial dependency among census tracts. All models were adjusted for the following covariates: % NH White, % NH Black, % Hispanic, low-income census tract status, per capita grocery store availability, % park space, walkability index, and population density (i.e., number of people per square mile). In addition, we used ordinary least squares (OLS) models to examine associations between violent crime rate and our two outcome measures stratified by racial/ethnic composition of residents. We ran OLS models among majority NH White tracts, majority NH Black tracts, majority Hispanic tracts, and racially diverse tracts separately. All OLS models were adjusted for the same list of covariates.
Results
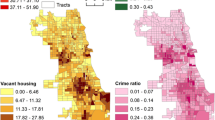
Figure 1 presents the bivariate maps generated to visualize the spatial distribution of violent crime rate relative to the prevalence of physical inactivity and obesity among adults in Chicago, IL. Darker colored census tracts are those in the highest tertiles for violent crime rate and the outcome variables (i.e., % physical inactivity and % obesity). Many of the census tracts in the highest tertile for violent crime and the outcome measures are located on the city’s south and west sides. Table 1 displays descriptive characteristics of census tracts in Chicago, IL. We calculated the median violent crime rate among all census tracts to be 1.5 per 1,000 persons with the minimum being 0.2 and the maximum being 25.3. Median % physical inactivity and % obesity were 29.3% and 32.5%, respectively.

Bivariate maps displaying the spatial distribution of violent crime rate relative to physical inactivity and obesity prevalence in Chicago, IL. Bivariate maps were created using ArcGIS Pro 2.6.1. Geographic units reflect census tracts in Chicago, IL (N = 798). Crime rate represents number of police-reported violent crimes per 1,000 residents in 2018. Physical inactivity and obesity represent prevalence rates (%) among adults (age ≥ 18) in 2018. Color blocks represent tertiles based on the empirical distribution of each variable
The results from the Kruskal–Wallis tests indicated that estimates for the outcome measures were different given the racial/ethnic composition of community residents (p < 0.001 for both). While the median violent crime rate was 0.6 per 1,000 persons in majority NH White census tracts, it was 4.7, 1.4, and 0.9 among majority NH Black, majority Hispanic, and racially diverse tracts, respectively. Median % physical inactivity was 17.9% among majority NH White tracts, but 35.9%, 32.6%, and 25.3% among majority NH Black, majority Hispanic tracts, and diverse tracts, respectively. Median % obesity was 23.7% among majority White tracts, but 43.5%, 34.0%, and 28.2% among majority NH Black, majority Hispanic, and racially diverse tracts, respectively. Median estimates for covariates also varied by racial/ethnic composition of residents.
Table 2 presents results from regression models assessing associations between violent crime rate and % physical inactivity by racial/ethnic composition of census tract residents. The spatial error regression model indicated that violent crime rate (β = 0.29; SE = 0.06; p < 0.001) was positively associated with % physical inactivity among all Chicago tracts after adjusting for covariates and accounting for the spatial dependency of adjoined tracts. OLS regression models indicated that violent crime rate was positively associated with % physical inactivity among majority NH Black tracts (β = 0.53; SE = 0.08; p < 0.001) and Hispanic tracts (β = 0.55; SE = 0.22; p = 0.01) after adjusting for covariates. We observed no association between violent crime rate and % physical inactivity among majority NH White tracts and racially diverse tracts. However, walkability index was negatively associated with % physical inactivity among majority NH White tracts. Low-income census tract status was significantly associated with % physical inactivity in all models.
Table 3 contains results from regression models examining associations between violent crime rate and % obesity by racial/ethnic composition of census tract residents. Again, the spatial error regression model indicated that violent crime rate (β = 0.31; SE = 0.06; p < 0.001) was positively associated with % obesity among all Chicago census tracts. OLS regression models examining associations by racial/ethnic composition of tract residents indicated that violent crime rate was positively associated with % obesity among majority NH Black tracts (β = 0.37; SE = 0.07; p < 0.001) and Hispanic tracts (β = 0.48; SE = 0.20; p = 0.01). Similar to % physical inactivity, we observed no association between violent crime rate and % obesity among majority NH White tracts and racially diverse tracts. However, walkability index was negatively associated with % obesity among majority NH White tracts. Low-income census tract status was associated with % obesity in all models.
Discussion
We aimed to examine violent crime rate at the census tract-level in Chicago, IL, and its association with the prevalence of obesity and physical inactivity among adults after controlling for sociodemographics and built environment features (e.g., grocery store availability, park space, walkability). Furthermore, we aimed to assess differences in associations given the racial/ethnic composition of residents. Our analyses indicated that violent crime rate was significantly associated with adult physical inactivity and obesity at the census-tract level after controlling for covariates. As violent crime rate increased, the prevalence of physical inactivity and obesity, on average, increased as well. These findings align well with other studies that have examined these associations at either the individual or the community levels.
Several prominent studies have evaluated the influence of violence, both perceived and objectively measured, on physical activity levels, behaviors (e.g., walking), and risk of obesity [17,18,19,20,21,22,23,24,25,26,27,28]. For example, a meta-analysis by Rees-Punia et al. 2018, which summarized findings across 16 published studies, indicated that feeling safe from crime is associated with greater odds of achieving high physical activity levels [17]. Bennett et al. (2007) reported that low-income women living in Boston who reported feeling unsafe in their neighborhood walked significantly fewer steps per day [18]. Assari et al. (2016) documented a significant association between fear of neighborhood violence among African American girls and higher BMI in early adulthood [23]. In regards objectively measured crime, Kerr et al. (2015) found that police-recorded crime, specifically murder, was associated with declines in transport walking over time among Chicago residents [21]. Tung et al. (2018) reported that violent crime rates were associated with obesity and high blood pressure in a high poverty area of Chicago [27]. Overall, these findings demonstrate a consistent knowledge base on the role of violence in increasing risk of physical inactivity and obesity.
Less is known about variations in these associations across communities given their racial/ethnic composition. The racial/ethnic composition of residents is an important factor to consider when evaluating the health effects of violent crime at the community level. Chicago is one of the most segregated urban centers in the USA, with high levels of black-white segregation after controlling for socioeconomic status [39]. Furthermore, Chicago’s racial segregation has been linked to historical inequities in opportunities, resources, and community amenities [39]. If violence is a manifestation of structural inequities that disproportionately affect communities of color, it is important to consider the role of community racial/ethnic composition when evaluating community-level disparities in physical inactivity and obesity.
In the current study, we found that the strength of associations varied given the racial/ethnic composition of residents. Violent crime rate was significantly associated with the prevalence of physical inactivity and obesity among tracts where majority of residents are NH Black or Hispanic. Associations were stronger (i.e., p < 0.001) among majority NH Black tracts, specifically. Rates for violent crime, physical inactivity, and obesity were relatively low in majority NH White and racially diverse tracts in comparison to majority NH Black and Hispanic tracts. These findings align with existing literature that reports higher rates of obesity and lower rates of leisure time physical activity among NH Black and Hispanic adults in the USA [27, 28, 40]. NH White and racially diverse tracts, on average, had higher median income, more park space, and a higher walkability score. These findings provide some insight to the long-standing structural inequities that exist in Chicago, IL, across communities. Few majority NH White tracts had median incomes below the city’s median, which challenged our ability to examine the role of racial/ethnic composition and the intersection of neighborhood socioeconomic advantage. The literature on this topic is consistent; prior studies have linked violent crime to physical activity behaviors and obesity risk in a variety of populations and settings [17,18,19,20,21,22,23,24,25,26,27,28]. Therefore, we believe that associations between violent crime, physical inactivity, and obesity would be significant in majority NH White tracts that are low-resourced and disadvantaged. Additional research is needed to test this hypothesis and advance the field’s understanding of structural drivers of violence, physical inactivity, and obesity.
This study adds to the current literature on the influence of violent crime on health and health behaviors. Findings may be useful to public health researchers and organizations working to document and address structural barriers to health in large urban centers, particularly those with high crime rates and high levels of racial segregation. Since violent crime is a structural barrier to maintaining healthy lifestyle behaviors, future policy, systems, and environmental change (PSE) interventions aimed at reducing physical inactivity and/or obesity should consider the role of community violence and other threats to public safety. To ensure the success of these interventions, researchers should examine relevant socioeconomic and environmental factors that contribute to violence such as urban blight (i.e., poor or decaying community infrastructure) [12, 14, 41]. Residing in a community that lacks adequate and equitable infrastructure can increase risk of not only obesity and physical inactivity, but chronic stress and poor dietary intake as well [42]. Improving the quality of community infrastructure (e.g., sidewalks, crosswalks, traffic-calming devices, bike lanes, lighting, and park space) and ensuring equitability across communities may encourage low-cost and accessible physical activities, such as walking, physical activity for transportation, and public park use [41].
Lastly, future endeavors to increase physical activity and prevent obesity important stakeholders such as community residents and local law enforcement agencies. Researchers should center residents in the development process by consulting and engaging with local community organizations [43]. Engaging the community early, often, and consistently can catalyze the community’s sense of ownership and support program sustainability [43]. Furthermore, future interventions should explore how public health entities and law enforcement agencies can collaborate to address violent crime and improve community health [44]. Interventions that position public safety as a key component are more likely to improve the community’s perceptions of safety, collective efficacy (e.g., social cohesion), and police legitimacy (e.g., rebuilding trust in the police), which can increase engagement in healthy lifestyle behaviors among community members [45].
This study has strengths and limitations. The data sources were a strength because they provided detailed information on sociodemographic, health, and environmental measures, which permitted a robust analysis at the census tract level. However, given differences in the availability of certain datasets, not all of the data years correspond to 2018. The park district boundaries data is from 2016 and the walkability index data is from 2017. Overall, we do not believe that park space and walkability scores in Chicago, IL, changed significantly from 2016 to 2018 to have affected our results. Another key limitation is the ecological and cross-sectional nature of this study. We did not examine individual-level data, so we cannot describe the influence of violent crime on the health and health behaviors of Chicago residents at the individual level. All findings from this analysis should be interpreted at the census tract level. We did not evaluate longitudinal associations, so we are unable to comment on temporality. Many of the research studies in this space have employed a cross-sectional study design [18,19,20, 22, 23]. Future studies should assess the longitudinal effects of violent crime on physical activity behaviors and obesity status. Due to the nature of the physical inactivity variable, we were unable to examine the prevalence of adults who do NOT meet CDC guidelines separately from those who reported no leisure-time physical activity. Having a variety of variables that represent various forms of physical inactivity would have made this analysis more robust. Furthermore, findings represent Chicago, IL, USA, only; they may not be applicable to other cities or countries.
In summary, we found that violent crime rate is significantly associated with the prevalence of physical inactivity and obesity at the census tract level in Chicago, IL. We found significant differences in associations across tracts given the racial/ethnic composition of community residents with stronger associations observed among majority NH Black tracts compared to Hispanic and NH White tracts. These findings underscore the need to further study violence as a structural barrier to maintaining a healthy lifestyle in large urban centers. Future research studies and health programming efforts should consider structural drivers of violence in urban communities: blight, social cohesion, police-community relations, etc. By studying these factors, the field will gain better perspective on how violence affects lifestyle behaviors and obesity risk.
Data Availability
All data used for this research project are available to the public online. Website links to the data sources are provided in the reference list.
References
Dahlberg LL, Mercy JA. History of violence as a public health problem. Virtual Mentor. 2009;11(2):167–72.
Wolf A, Gray R, Fazel S. Violence as a public health problem: an ecological study of 169 countries. Soc Sci Med. 2014;104(100):220–7.
The Marshall Project. New FBI Data: Violent crime still falling. 2019. Available at: https://www.themarshallproject.org/2019/09/30/new-fbi-data-violent-crime-still-falling. Accessed January 22, 2021.
Brennan Center for Justice. Takeaways from 2019 crime data in major American cities. 2019. Available at: https://www.brennancenter.org/our-work/analysis-opinion/takeaways-2019-crime-data-major-american-cities. Accessed January 31, 2021.
Premkumar, D. Public scrutiny, police behavior, and crime consequences: evidence from high-profile police killings. Public Policy Institute of California. 2022. Available at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3715223. Accessed December 21, 2022.
Chicago Department of Public Health. Healthy Chicago 2025: Data Compendium. 2019. Available at: https://www.chicago.gov/content/dam/city/depts/cdph/CDPH/Healthy_Chicago_2025_Data-Compendium_10222019.pdf. Accessed January 22, 2021.
Walker GN, McLone S, Mason M, Sheehan K. Rates of firearm homicide by Chicago region, age, sex, and race/ethnicity, 2005–2010. J Trauma Acute Care Surg. 2016;81(4 Suppl 1):S54–60.
Riddell CA, Harper S, Cerda M, Kaufman JS. Comparison of rates of firearm and nonfirearm homicide and suicide in black and white non-Hispanic men, by U.S. State. Ann Intern Med. 2018;168(10):712–20.
Krivo LJ, Peterson RD, Kuhl DC. Segregation, racial structure, and neighborhood violent crime. Am J Sociol. 2009;114(6):1765–802.
Rivara F, Adhia A, Lyons V, Massey A, Mills B, Morgan E, Simckes M, Rowhani-Rahbar A. The effects of violence on health. Health Aff. 2019;38(10):1622–9.
Sumner SA, Mercy JA, Dahlberg LL, Hillis SD, Klevens J, Houry D. Violence in the United States: status, challenges, and opportunities. JAMA. 2015;314(5):478–88.
Branas CC, Kondo MC, Murphy SM, South EC, Polsky D, MacDonald JM. Urban blight remediation as a cost-beneficial solution to firearm violence. Am J Public Health. 2016;106(12):2158–64.
Jennings JM, Milam AJ, Greiner A, Furr-Holden DM, Curriero FC, Thornton RJ. Neighborhood alcohol outlets and the association with violent crime in one mid-Atlantic City: the implications for zoning policy. J Urban Health. 2014;91(1):62–71.
Kondo M, Hohl B, Han S, Branas C. Effects of greening and community reuse of vacant lots on crime. Urban Stud. 2016;53(15):3279–95.
Bailey ZD, Krieger N, Agenor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389(10077):1453–63.
Anderson E, Durstine L. Physical activity, exercise, and chronic diseases: a brief review. Sports Med Health Sci. 2019;1(1):3–10.
Rees-Punia E, Hathaway ED, Gay JL. Crime, perceived safety, and physical activity: a meta-analysis. Prev Med. 2018;111:307–13.
Bennett GG, McNeill LH, Wolin KY, Duncan DT, Puleo E, Emmons KM. Safe to walk? Neighborhood safety and physical activity among public housing residents. PLoS Med. 2007;4(10):1599–607.
Evenson KR, Block R, Diez Roux AV, McGinn AP, Wen F, Rodríguez DA. Associations of adult physical activity with perceived safety and police-recorded crime: the multi-ethnic study of atherosclerosis. Int J Behav Nutr Phys Act. 2012;9:146.
Janke K, Propper C, Shields MA. Assaults, murders and walkers: the impact of violent crime on physical activity. J Health Econ. 2016;47:34–49.
Kerr Z, Evenson KR, Moore K, Block R, Diez Roux AV. Changes in walking associated with perceived neighborhood safety and police-recorded crime: the multi-ethnic study of atherosclerosis. Prev Med. 2015;73:88–93.
Ou JY, Levy JI, Peters JL, Bongiovanni R, Garcia-Soto J, Medina R, Scammell MK. A walk in the park: the influence of urban parks and community violence on physical activity in Chelsea, MA. Int J Environ Res Public Health. 2016;13(1):97.
Assari S, Moghani Lankarani M, Caldwell CH, Zimmerman MA. Fear of neighborhood violence during adolescence predicts development of obesity a decade later: gender differences among african americans. Arch Trauma Res. 2016;5(2):8–15.
Gooding HC, Milliren C, Austin SB, Sheridan MA, McLaughlin KA. Exposure to violence in childhood is associated with higher body mass index in adolescence. Child Abus Negl. 2015;50:151–8.
Powell-Wiley TM, Wong MS, Adu-Brimpong J, Brown ST, Hertenstein DL, Zenkov E, Ferguson MC, Thomas S, Sampson D, Ahuja C, Rivers J, Lee BY. Simulating the impact of crime on African American women’s physical activity and obesity. Obesity. 2017;25(12):2149–55.
Stolzenberg L, D’Alessio SJ, Flexon JL. The impact of violent crime on obesity. Soc Sci. 2019;8(12):329.
Tung EL, Wroblewski KE, Boyd K, Makelarski JA, Peek ME, Lindau ST. Police-recorded crime and disparities in obesity and blood pressure status in Chicago. J Am Heart Assoc. 2018;7(7): e008030.
Yu E, Lippert AM. Neighborhood crime rate, weight-related behaviors, and obesity: a systematic review of the literature. Sociol Compass. 2016;10(3):187–207.
Chicago Police Department. Citizen law enforcement analysis and reporting map (CLEARmap) Application. 2021. Available at: https://home.chicagopolice.org/services/clearmap-application/. Accessed June 13, 2020.
Federal Bureau of Investiagtion. Violent Crime. 2018. Available at: https://ucr.fbi.gov/crime-in-the-u.s/2018/crime-in-the-u.s.-2018/topic-pages/violent-crime#:~:text=In%20the%20FBI's%20Uniform%20Crime,force%20or%20threat%20of%20force. Accessed July 11, 2020.
Centers for Disease Control and Prevention. PLACES: local data for better health. 202. Available at: https://www.cdc.gov/places/index.html. Accessed June 25, 2020.
Centers for Disease Control and Prevention. Physical activity basics. 2020. Available at: https://www.cdc.gov/physicalactivity/basics/index.htm. Accessed January 29, 2021.
Centers for Disease Control and Prevention. Body mass index (BMI). 2022. Available at: https://www.cdc.gov/healthyweight/assessing/bmi/index.html. Accessed January 29, 2021.
U.S. Census Bureau. 2021. Available at: https://www.census.gov/. Accessed June 23, 2020.
Chicago Data Portal. Grocery Store Status. 2020. Available at: https://data.cityofchicago.org/Health-Human-Services/Grocery-Store-Status/3e26-zek2. Accessed July 14, 2020.
Chicago Data Portal. Chicago park district park boundaries. 2020. Available at: https://data.cityofchicago.org/Parks-Recreation/Parks-Chicago-Park-District-Park-Boundaries-curren/ej32-qgdr. Accessed September 2, 2020.
Environmental Protection Agency. Smart location mapping: interactive maps and data for measuring location efficiency and the build environment. 2021. Available at: https://www.epa.gov/smartgrowth/smart-location-mapping. Accessed August 25, 2020.
Esri. Making Bivariate Choropleth Maps with ArcMap. 2021. Available at: https://www.esri.com/arcgis-blog/products/mapping/mapping/making-bivariate-choropleth-maps-with-arcmap/. Accessed April 27, 2021.
Hendricks K, Lewis AE, Arenas I, Lewis DG. A tale of three cities: the state of racial justice in Chicago report. UIC Institute for Research on Race & Public Policy. 2017. Available at: https://www.researchgate.net/publication/323151248_A_Tale_of_Three_Cities_The_State_of_Racial_Justice_in_Chicago_Report. Accessed January 16, 2021.
Moore LV, Harris CD, Carlson SA, Kruger J, Fulton JE. Trends in no leisure-time physical activity—United States, 1988–2010. Res Q Exerc Sport. 2012;83(4):87–91.
Zenk SN, Pugach O, Ragonese-Barnes M, Odoms-Young A, Powell LM, Slater SJ. Did playground renovations equitably benefit neighborhoods in Chicago? J Urban Health. 2021;98:248–58.
Pickett S, McCoy TP, Odetola L. The influence of chronic stress and emotions on eating behavior patterns and weight among young African American women. West J Nurs Res. 2020;42(11):894–902.
Cyril S, Smith BJ, Possamai-Inesedy A, Renzaho AMN. Exploring the role of community engagement in improving the health of disadvantaged populations: a systematic review. Glob Health Action. 2015;8(1):29842.
White C, Weisburd D. A co-responder model for policing mental health problems at crime hot spots: findings from a pilot project. Policing. 2018;12(2):194–209. https://doi.org/10.1093/police/pax010.
Dong B, White CM, Weisburd DL. Poor health and violent crime hot spots: mitigating the undesirable co-occurrence through focused place-based interventions. Am J Prev Med. 2020;58(6):799–806.
Acknowledgements
The authors have no acknowledgements.
Funding
The research reported in this paper was not supported by a grant or funding source.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Singleton, C.R., Winata, F., Parab, K.V. et al. Violent Crime, Physical Inactivity, and Obesity: Examining Spatial Relationships by Racial/Ethnic Composition of Community Residents. J Urban Health 100, 279–289 (2023). https://doi.org/10.1007/s11524-023-00716-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-023-00716-z