
Abstract
Adult drowning is a complex and multifactorial public health challenge requiring community, national and global efforts to mitigate impacts. This study updates the evidence base for public health interventions that address adult fatal and non-fatal drowning. A systematic review was undertaken of the peer-reviewed literature for English-language primary studies published between 2011 and 2021describing a drowning intervention with adults. Twenty-two studies were included. Most studies (n = 16) were conducted in high-income countries. Yearly trends in drowning prevention intervention publications were analysed with 2015 (n = 6) the peak publishing year. Over half of the study designs were pre-post (n = 15). Intervention duration ranged from 4 hours to 11 years. Ten studies described either behaviour change theory or formative evaluation to inform design. Thirteen studies targeted interventions at a population level, seven at a group level and two at individual level. Studies identified a range of prevention strategies, categorised as behavioural (n = 9) (e.g., swimming lessons), socio-ecological (n = 8) (e.g., mandatory personal flotation devices) and mixed (n = 5) (e.g., awareness campaign and barriers to prevent access to water). A range of outcomes were described including changes in awareness, water safety knowledge, attitudes, water safety behaviours and skills, environmental, policy and regulation changes and drowning rates. Findings indicate a small but important increase in the evaluation and publication of effective interventions to prevent adult drowning. The complexity of the issues surrounding drowning requires multi-strategy and context -specific adult focused prevention interventions. Contemporary evidence that identifies effective interventions that contribute to prevention efforts is an essential first step in addressing the challenge.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Drowning is a global public health challenge. In 2019, more than 230 000 people drowned, with the majority (90%) occurring in low-income and middle-income countries (LMICs) [1, 2]. Close to two-thirds of all reported drowning deaths involved those aged 15 or older [1]. Both fatal and non-fatal drowning have significant impacts, including loss of household income and support, family breakdown and increased burden of care for survivors [3,4,5,6].
Drowning prevention in adults is a complex, multifaceted public health issue [7, 8]. Some risk factors (age, male gender, ethnicity, low socioeconomic status, and the use of alcohol) [9, 10] are consistent globally. However, others, for example weather, boat carrying capacity and watercraft design are specific to local social and cultural environments [11, 12].
Adult risk factors can be categorised as either behavioural (e.g., alcohol use, swimming alone and wearing a lifejacket) or socio-ecological factors (for example, water safety literacy, unsafe watercraft and unprotected infrastructure and equipment) [8, 13,14,15]. Globally, male drowning risk is high, with twice the overall mortality rate of females [16]. This disparity is primarily due to greater exposure to water and engagement in practices and behaviours which may place them at higher risk [8, 17, 18]. In high-income countries (HICs), males participate more frequently in recreational swimming, boating, and fishing [14, 19]. Risk is exacerbated by specific behaviours such as swimming alone, not wearing a personal floatation device (PFD) when boating or rock fishing, and alcohol consumption [8, 13, 14, 20, 21]. In contrast, in LMICs, males are exposed daily to natural waterbodies as a source of livelihood, using water transport to and from work, including in vessels that are often overcrowded and poorly maintained [12, 22, 23]. Age is also a significant factor in drowning risk. For example, young people (particularly males aged over 16 years) in HICs are at greater risk of drowning, attributed to risk-taking behaviours, peer pressure, poor aquatic competency and alcohol use [8, 21, 24, 25]. In contrast, for older adults (65 years and over) in HICs, risks relate to bathing, falls into water, poor health, alcohol consumption, medication use and lack of safety preparation around natural water bodies or during recreational activities [26, 27].
In 2016, the authors published a systematic review of adult drowning prevention interventions [8]. Only six studies met the inclusion criteria, briefly, three studies reported on interventions using educational strategies, one reported an environmental change intervention, and two studies reported legislative change interventions – all studies were located in HICs [8]. Studies were of mixed design and quality, with limited reference to theory or formative research. The 2016 review called for more robust studies underpinned by evidence-informed health promotion approaches [8]. More recently, the literature has seen an increase in the publication of research focusing on drowning prevention [28] supported by the impetus from the 2021 United Nations (UN) Global Charter for Drowning Prevention [29] which called for strengthened multi-strategy, multisectoral actions in drowning prevention around the globe. This updated systematic review aimed to assess the contemporary evidence base for adult -focused, public health interventions that address fatal and non-fatal drowning.
Methods
The review replicated the steps for the previous review outlined by Leavy, Crawford [8] and Crawford, Leavy [30], in line with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [31].
Study Setting and Participants
The study setting and participants matched the description provided in the previous adult review [8]. Briefly, we analysed public health, primary studies, focusing on drowning interventions designed to prevent adult fatal or non-fatal drowning. For the purposes of the review, adults were defined as individuals over the age of 18. Eighteen years of age has been designated as the age at which childhood ends by the UNICEF Convention on the Rights of the Child [28]. Interventions aimed at both children/young people and adults were included where there was clear reporting on the impact of the intervention on adults.
Criteria for Inclusion
Included articles met the following criteria: peer-reviewed, published in English between 2011 and 2021 that described and evaluated adult drowning primary prevention interventions targeting an individual, and/or group and/or population level. We included experimental and observational studies, randomised and non-randomised controlled trials, cohort studies, case-control studies, cross-sectional studies, retrospective analysis, and qualitative studies that evaluated primary adult drowning prevention interventions/strategies [8, 30] See Table 1. As established by the previous review, primary prevention strategies were those that eliminate or reduce causes of poor health, and/or promote protective factors. Secondary and tertiary intervention/s (those that include early detection, delaying complications, management, and rehabilitation, which occur after the possibility of prevention e.g., resuscitation) and reviews were excluded [8, 30].
Search Strategy
The research team searched 15 databases: PubMed; JSTOR; CINAHL; EMBASE; ERIC; ProQuest; PsycINFO; ScienceDirect; Scopus; Global Health; Web of Science; Current Contents; Wiley Online Library; Medline; and Sport Discus. Keywords and MESH terms were:
-
1.
drown* adjacent to (prevent* or safety) within 3 words [MESH: Drowning/ pc [Prevention & Control].
-
2.
interven* OR evaluat* OR “best practice” OR “good practice” OR “best practise” OR “good practise” OR “health promot*” OR “public health” OR polic* OR program* OR research OR prevent* OR education OR curriculum [MESH: Health Education/ and Preventive Health Services/].
Outcome Measures
Outcome measures included: drowning rates; water safety behaviour changes, or changes in behavioural intention or drowning awareness, knowledge, attitudes, water safety policy and legislation; changes to environment; and water safety skills.
Selection of Articles, Screening and Quality Appraisal
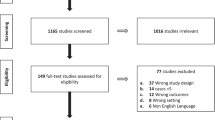
Endnote X9 [32] and Rayyan.AI [33] supported the selection and screening process [34]. Duplicates were removed, and two research assistants (AV) and (TG) screened article titles and abstracts for relevance against the inclusion criteria using-Rayyan.AI [33], a tool for screening and record-keeping to facilitate researcher collaboration. Excluded publications were scanned, and one research assistant (TG) randomly cross-checked 10% to identify any selection anomalies. The full-text articles from relevant studies that met the inclusion criteria were retrieved and reviewed by three reviewers (AV, JL & GC) to confirm eligibility for inclusion (see Fig. 1). Reviewer discussion resolved inconsistencies. The reference lists of all included articles were hand-searched for any relevant studies that had not been previously retrieved.
Twenty-six studies were quality appraised by two reviewers (JL and ND), using a purposively tailored quality appraisal checklist adapted from the MetaQAT framework [35]. The tool consists of four domains: relevancy; reliability; validity; and applicability [35]. Appraisers allocated a score to each of the nine criteria in the domains, whereby: Met the criteria = 2, Not sure/Unclear = 1; Did not meet the criteria = 0. A maximum score of 18 was allocated. Studies were then categorised based on the overall score, ≤ 9 = low quality, 10–14 = medium quality; and 15–18 = high quality. After the quality appraisal, four (n = 4) studies were reviewed independently by GC and deemed unsuitable for inclusion. A final sample of n = 22 studies were included in the revie.

Systematics Review Flow Chart following PRISMA 2020 flow diagram for new systematic reviews template [31]
Data Extraction, Analysis and Synthesis
Data extraction replicated the procedure from the previous review. Briefly, descriptive and outcome data for all included articles were identified and recorded using a standardised data extraction form by two reviewers (AV, ND) and checked by a third reviewer (CG). Full-text articles were read and annotated to extract information under each of the following headings: author (year) & aims and objective; location & sample (n); recruitment & response rate; intervention level (individual, group, population), strategy type (behavioural defined as actions that individuals take concerning drowning prevention [36]; or socio-ecological defined as part of the social, physical and policy environment [37]), activity type (e.g. education, environmental, regulatory); duration; behaviour theory (BT) and formative research (FR); evaluation design; measures; ethical approval; and impacts/outcomes. Results were reviewed by the authors (JEL, GC, CG) for consistency.
Basic reporting of “pooled” data on age, gender and key findings are included. No meta-analyses were conducted due to the considerable heterogeneity across the studies.
Results
Setting, Duration and Evaluation Design
Twenty-two studies were included in the review (Table 2). The majority (n = 16) [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53] were from HICs; six [54,55,56,57,58,59] were from LMICs. Australia (n = 7) [38, 39, 43, 46, 48, 52, 53] and the US (n = 6) [40,41,42, 47, 49, 51] were the two most represented geographical locations, representing over half of included studies.
The intervention study designs included pre-post studies (n = 15) [39, 41, 42, 45, 46, 49,50,51, 54, 57,58,59] [38, 55, 56], cross-sectional studies (n = 4) [43, 44, 48, 52], an observational study [40], a retrospective analysis [47] and a qualitative study [53].
There were two female-gender specific studies [53, 59]. The duration of drowning interventions ranged from 4 to 5 hours [46] to 11 years [38] while sample sizes ranged from 13 [54] to > 75 000 [42]. Ethical approval was reported for 15 studies [38,39,40,41, 43, 46, 48, 50,51,52,53, 55,56,57,58]. Yearly trends in drowning prevention intervention publications were analysed (Fig. 2). demonstrating one peak publishing year (2015).

Yearly Trend of Adult Drowning Prevention Intervention Studies
Drowning Prevention Strategies
Two studies [50, 59] presented interventions targeting individuals while seven studies presented interventions targeting groups [44,45,46, 48, 49, 54]. All but one [49] of these studies utilised behavioural strategies (Table 3). Behavioural activities were reported as educational, involving swimming lessons [46, 48, 50, 53, 54, 59] or educational materials (i.e., safety messages via field officers) [44, 45]. The study by Schwebel et al. (2011) used a regulatory audit to assess lifeguard behaviour.
The remaining thirteen studies [38,39,40,41,42,43, 47, 51, 52, 55,56,57,58] reported on interventions targeting a population, and included the use of behavioural approaches [52], socio-ecological approaches [38,39,40,41, 43, 47, 51] or a mix of strategy types [42, 55,56,57,58]. For example, the population-level behavioural intervention by Warton and Brander (2017) evaluated the effectiveness of the television show Bondi Rescue on water safety knowledge. The four studies involving both behavioural and socio-ecological interventions used a combination of educational material (i.e., drowning awareness campaigns) and changes in environment (i.e., barriers to water, increased lifejackets available) [55,56,57,58], with one study [42] comparing differences between an educational or regulatory intervention. Of the studies applying a socio-ecological approach, five studies were regulatory, involving the introduction of mandatory personal floatation devices (PFDs) [38,39,40] or other regulations [47, 51]. Two studies were environmental, involving signage [41, 43].
Behavioural Theory and Formative Research
Six studies (27%) reported the use of behavioural theory [41, 43, 44, 46, 49, 51, 53]. Two studies used the Health Belief Model [60], one applied it to swimming classes [53] and the other to lifeguard surveillance [49]. Other theories included the Socio-Ecological Model [51], Protection Motivation Theory [44], Theory of Planned Behaviour [53], General Deterrence Theory [41], Communication-Human Information Processing Model [43] and general considerations of pedagogical approaches [46].
Four studies (18%) described using some form of formative research to inform the intervention design and delivery and profile the target audience. Methods included a cross-sectional survey [44] and focus group discussions [51] with community members. Sansiritaweesook et al. (2015) reported using a two-month situational analysis before intervention development. Davoudi-Kiakalayeh et al. (2013) scaled their intervention based on a previous pilot intervention in the community.
Intervention Outcomes
Outcomes described included: changes in awareness, water safety knowledge, attitudes, water safety behaviours and skills, together with environmental, policy and regulation changes and drowning rates. All but two studies reported some intervention effect [43, 50]. Scurati et al. (2019) assessed two different forms of feedback (traditional or through mobile devices) in a breaststroke swim program but found no significant differences. A cross-sectional survey by Matthews et al. (2014) asked beachgoers about hazard signage but found better knowledge of hazards on beaches without signs. Savage and Franklin (2015) found culturally and linguistically diverse (CaLD) participants more likely to complete a swimming and water safety course when using specific Indigenous/ CaLD resources than with the standard course, but less likely to complete the Korean course compared to the standard course. Six studies measured changes across multiple outcome categories [38, 44,45,46, 57, 58].
Eight studies (36%) measured water safety behavioural changes, with five reporting increases in the use of PFDs or lifejackets [38,39,40, 42, 44]. Other reported behavioural changes included reduced water entry [41], reduced incidence of risky swimming behaviour [58], and improved lifeguard-looking behaviour [49]. Eight studies (36%) measured changes in water safety skills, with six describing improvements in swimming ability [48, 50, 53, 54, 57, 59]. The study by Petrass et al. (2018) measured simulated rescue competency, and the two studies by Sansiritaweesook and colleagues (2015a, 2015b) reported increases in the proportion of volunteer rescue personnel with resuscitation training [57, 58].
Six studies (27%) assessed changes in drowning rates [38, 47, 55,56,57,58]. Four studies assessed knowledge, with three relating to rescue knowledge [45, 46, 52], and the study by Matthews et al. (2014) reporting no change in hazard knowledge. Other outcomes included environmental changes (increased lifejackets and rescue boats) [58], improved attitudes towards rescue [45], and increased number of water safety policies and regulations [51].
Self-reported Study Limitations
Four studies did not report any limitations [43, 46, 52, 59]. Self-reported limitations relating to recruitment and participants included: a low response rate [48] and a small sample size [48,49,50, 53], convenience sampling [44, 45, 53], and English-only survey instruments [45, 48]. Limitations relating to study design included: short-term intervention [54], no control or comparison group [38, 55, 56], self-reported behaviour [44], selection bias [47], cross-contamination between groups [58], and lack of generalisability to other settings/groups [57]. Studies using observational data noted the potential for observational bias or misclassification of data [39, 40, 42, 61]. Girasek (2019) stated that the introduction of a camera may have influenced behaviour and enhanced the effectiveness of the intervention.
Discussion
This study updates a previous systematic review undertaken in 2016 [8]. This review noted a three-fold increase in studies (from six to twenty-two articles), published between 2011 and 2021, that reported on public health interventions for adults. Of note, a recent bibliometric analysis found 39% of drowning research publications were from Australia and the US [28]. We found similar results with 37.5% of intervention studies from Australia and the US, and most (n = 16) from HICs. Interventions varied by intervention level, duration and design across the 22 studies. Nearly half of studies described the use of behavioural theory or formative research, and all but two interventions reported some intervention effect. Overall, the review found some positive shifts in the design and evaluation of adult focused drowning prevention interventions highlighting the vital contribution of research and evidence for interventions delivered across countries and communities globally.
Promisingly, and in line with contemporary health promotion and prevention approaches [62], more than half (n = 13) of the included studies in this review focused on population-level interventions using a socio-ecological or mixed strategy approach. In comparison, our previous review found a predominance of behavioural-only strategies emphasising education [8]. While behavioural interventions have merit, changes are often short-term. They may have limited impact on longer-term, population-level outcomes [63], such as fatal drowning events. In comparison, socio-ecological strategies often involve sustained interventions, such as regulatory or environmental changes, that are more likely to produce population-level outcomes [64]. Regulatory or environmental changes are more likely to be cost-effective long term [65] and translate to sustained behaviour change [66]. In this review, six studies assessed changes in drowning rates following either the introduction of regulatory PFD usage or environmental changes (e.g., increased barriers to water or availability of rescue equipment), with all demonstrating a considerable reduction in the number of drownings in the population sustained over time. The novel study by Girasek (2019) used signage and a considerable fine to achieve change. The study is an important reminder that multi-strategy prevention efforts targeting both the person at risk and structural considerations such as using regulatory options are more likely to be successful than programs relying on a single strategy. This finding is consistent with the broader literature on health promotion and prevention [62, 67]. By comparison, studies in this review focusing on behavioural-only strategies generally reported on short-term changes, such as knowledge and swimming skills, often amongst a small sample size and within a short time frame.
Socio-ecological strategies may also be more effective than behavioural-only campaigns for some behavioural measures [67]. For example, Mangione and Chow (2014) observed differences in lifejacket use between an educational lifejacket campaign and mandatory lifejacket regulations. Mandatory regulations increased lifejacket use by more than 50%, whilst the educational campaign increased lifejacket use by only 2% and was unsustained. While the authors could not accurately estimate the costs of implementing campaigns, they noted that the educational campaign required sizeable ‘new’ expenses. At the same time, mandatory regulation added little cost to existing activity [42]. Similarly, Chung et al. (2014) observed lifejacket use was considerably higher among boat users who were legally required to wear a lifejacket (96.8%) compared with boat users not wearing a lifejacket (21.1%). Comparatively, after a decade-long educational campaign in New Zealand, Moran et al. (2017) found only 40% of rock-fishers self-reported always/often wearing a lifejacket. A recent similar project in Victoria, Australia reported that their three-year educational campaign with rock fishers produced no change in lifejacket use [68]. The findings of the review highlight the availability, and regulation of lifejacket use as a critical and cost-effective approach to drowning prevention.
Those in public health have long advocated for the use of theory to plan, deliver, and evaluate interventions [69]. In this review, the use of behavioural theory and formative research was limited, similar to the findings of our previous reviews with adults [8] and children [7]. Studies used a range of theory with varying levels of application. In general theories were mentioned, but description of their application – to design and evaluation – was limited. Of note, one recent Australian qualitative study [53] described and mapped constructs from two theories, Health Belief Model [70] and the Theory of Planned Behaviour [71]to guide the focus group and individual interview question guide. This study provides an exemplar for future drowning prevention evaluation research. Similarly, Stempski et al. (2015) used the Socio-Ecological Model [72] to outline how policy and systems at a community level may help to improve the factors that influence swimming and water recreation. The use of formative research was limited in included studies, despite being a critical component of effective public health practice [73]. The use of theory has been highlighted as instructive to improve our understanding of the complexities of health behaviour and the environment which influences them [74].
Studies mostly reported positive outcomes from their interventions. Our previous review called for an increase in appropriate study designs, objective, valid and reliable measures and quality evaluations over a sufficient period [8]. The current review found the most frequently reported outcomes included water safety behaviour (mainly the use of PFDs) and water safety skills (predominately swimming skills). These outcomes were mainly evaluated through a pre-post study design, using observational data. While issues of observational bias and misclassification of data were reported, they may be more reliable than self-reporting of behaviour and skills [74]. However, several of these studies had relatively short timeframes of less than a few months [41, 45, 46, 49, 50, 54, 59] and/or were conducted with small samples [49, 50, 53, 54, 59], meaning it is unknown as to whether behaviour and skills were sustained over time [74], and likely to impact on both fatal and non-fatal drowning outcomes. Despite being published post the previous review, these studies do not incorporate previous recommendations. Promisingly, six studies measured changes in drowning rates, using a pre-post analysis to compare data across several years. All studies demonstrated a positive impact of interventions on drowning rates, though causation cannot be assumed. Only four studies used a cross-sectional design, measuring a mixture of knowledge, attitudes, skills and behaviour. Previous reviews have cautioned against reliance on self-report measures [7, 8, 24]. Overall, findings suggest incremental improvements in use of robust and standardised measures by researchers and practitioners, although improvements are warranted.
While almost 90% of drownings occur in LMICs [1, 2], the majority (n = 16) of articles included in this review were from HIC settings. Interventions in LMICs are delivered by a range of government and community-based agencies, that may not always have the capacity or resources for large-scale evaluation and knowledge translation [28, 75, 76]. Alternatively, knowledge translation may not be a priority or evaluation results may not be disseminated widely [77,78,79] or undertaken through other means, such as the grey literature [79, 80]. Of interest, a recent scoping review of the grey literature identified intersections for drowning prevention within global reports for occupational, environmental and urban health, refugee and migrant safety and disaster risk reduction, identifying potential partners and sectors to increase drowning prevention efforts [79] across a variety of settings. Additionally, while population approaches to drowning prevention are needed, there remains a role for targeted programs for potential at-risk groups, such as migrants or people from lower socioeconomic backgrounds [10, 53]. Three studies in this review focused on migrants [48, 53] or female non-swimmers [59]; however, the quality of design varied, sample sizes were small, and one study did not report an improvement [48]. Further evidence of approaches that work with different groups across different settings to address inequities in drownings is warranted.
Strengths and Limitations
This study updates a previous review of drowning prevention interventions amongst adults, totalling 31 years of peer-reviewed literature. Strengths include searching fifteen databases, providing a broad scope, and following procedures from previously published systematic reviews [7, 8]. Additionally, use of the MetaQAT tool for quality appraisal is viewed as a strength as it is a public health specific tool. A teams-approach was adopted to finalise article selection, minimising potential errors. Several limitations are noted. Included articles were restricted to the English language, and grey literature was excluded. We acknowledge that non-English articles and the grey literature may yield valuable information on drowning prevention interventions. Community-based agencies are likely to deliver most interventions but may be less likely to publish in a peer-reviewed forum; therefore, their contributions may have been excluded. Despite these limitations, this review provides a contemporary overview of drowning prevention interventions for adults in low-, middle- and high-income countries.
Conclusion
Drowning prevention in adults is a complex, multifaceted issue of public health significance but evidence for intervention development has been lacking This review updates the evidence base for adult-focused, public health interventions that address fatal and non-fatal drowning. Since our last review there has been a modest increase in the number of interventions published, together with some positive gains in design, delivery and evaluation over the past decade. Findings reinforce global calls for multi-level, multi-strategy approaches to intervention design, implementation and evaluation for maximum gains aligned with contemporary health promotion and prevention approaches.
Change history
24 February 2023
Missing Open Access funding information has been added in the Funding Note.
References
Franklin, R. C., et al. (2020). The burden of unintentional drowning: global, regional and national estimates of mortality from the global burden of Disease 2017 study. Injury Prevention, 26(Suppl 2), i83–i95.
Meddings, D. R., et al. (2021). Drowning prevention: turning the tide on a leading killer. The Lancet Public Health, 6(9), e692–e695.
Houser, C., Arbex, M., & Trudeau, C. (2021). Short communication: economic impact of drowning in the Great Lakes Region of North America. Ocean & Coastal Management, 212, 105847.
Mahony, A., et al. (2017). A thirteen year national study of non-fatal drowning in Australia: data challenges, hidden impacts and social costs. Royal Life Saving Society Australia.
Royal National Lifeboat Institute (2015). Estimating the Global Economic Cost of Drowning.
Whitworth, H. S., et al. (2019). Drowning among fishing communities on the Tanzanian shore of lake Victoria: a mixed-methods study to examine incidence, risk factors and socioeconomic impact. British Medical Journal Open, 9(12), e032428.
Leavy, J. E., et al. (2016). A review of drowning prevention interventions for children and young people in high, low and middle income countries. Journal of Community Health, 41(2), 424–441.
Leavy, J. E., et al. (2015). Recreational drowning prevention interventions for adults, 1990–2012: a review. Journal of Community Health, 40(4), 725–735.
Leavy, J. E. (2017). Drowning in International Encyclopedia of Public Health (Second edition), S Quan, Editor. Academic Press. p. 361–365.
Quan, L. (2014). Review of risk factors, in Drowning, J. Bierens, Editor. Springer Verlag: Berlin Heidelberg. p. 123–126.
Tyler, M. D., et al. (2017). The epidemiology of drowning in low-and middle-income countries: a systematic review. Bmc Public Health, 17(1), 1–7.
Lukaszyk, C., Ivers, R. Q., & Jagnoor, J. (2018). Systematic review of drowning in India: Assessment of burden and risk. Injury Prevention, 24(6), 451–458.
Petridou, E., & Klimentopoulou, A. (2006). Risk Factors for Drowning, in The Handbook of Drowning. p. 63–69.
ILS, World Drowning Report.International Life Saving Federation.
Rahman, F., et al. (2012). Cost-effectiveness of an injury and drowning prevention program in Bangladesh. Pediatrics, 130(6), e1621–e1628.
World Health Organization. Cause-specific mortality, 2000–2019 (2020). [cited 2022 14 Oct]; Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death.
WHO. (2014). Global report on drowning: preventing a leading killer. World Health Organization.
World Health Organization. Drowning (2021). [cited 2022 14 Oct]; Available from: https://www.who.int/news-room/fact-sheets/detail/drowning.
Royal Life Saving Society Australia. (2021). Royal Life saving National drowning Report 2021. Australia: Sydney.
Cortés, L. M., Hargarten, S. W., & Hennes, H. M. (2006). Recommendations for water safety and drowning prevention for travelers. Journal of Travel Medicine, 13(1), 21–34.
Leavy, J., et al. (2022). Drinking and swimming around waterways: the role of alcohol, sensation-seeking, peer influence and risk in young people. PLoSOne, 17(11), e0276558.
Miller, L., et al. (2019). Epidemiology, risk factors and measures for preventing drowning in Africa: a systematic review. Medicina, 55(10), 637.
Tyler, M. D., et al. (2017). The epidemiology of drowning in low- and middle-income countries: a systematic review. Bmc Public Health, 17(1), 413.
Wallis, B. A., et al. (2015). Interventions associated with drowning prevention in children and adolescents: systematic literature review. Injury Prevention, 21(3), 195–204.
Roberts, K., et al. (2021). A scoping review of female drowning: an underexplored issue in five high-income countries. Bmc Public Health, 21(1), 1–13.
Abercromby, M., et al. (2020). Who are the older adults who drown in western Australia? A cluster analysis using coronial drowning data. International Journal of Aquatic Research and Education, 13(1), 7.
Clemens, T., Peden, A. E., & Franklin, R. C. (2021). Exploring a hidden epidemic: drowning among adults aged 65 years and older. Journal of Aging and Health, 33(10), 828–837.
Scarr, J. P., & Jagnoor, J. (2021). Mapping trends in drowning research: a bibliometric analysis 1995–2020. International Journal of Environmental Research and Public Health, 18(8), 4234.
United Nations. Drowning is a leading cause of accidental death (2021). [cited 2022 14 Oct]; Available from: https://www.un.org/en/observances/drowning-prevention-day.
Crawford, G., et al. (2014). Development of a systematic review of public health interventions to prevent children drowning. Open Journal of Preventive Medicine, 4, 100–106.
Page, M. J., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj, 372, n71.
Clarivate (2020). Endnote X9. ; Available from: https://endnote.com/downloads.
Ouzzani, M., et al. (2016). Rayyan—a web and mobile app for systematic reviews. Systematic Reviews, 5(1), 210.
Hupe, M., & EndNote, X. (2019).Journal of Electronic Resources in Medical Libraries, 16:117–119.
Rosella, L., et al. (2016). The development and validation of a meta-tool for quality appraisal of public health evidence: Meta Quality Appraisal Tool (MetaQAT). Public Health, 136, 57–65.
Nutbeam, D., & Muscat, D. M. (2021). Health Promotion Glossary Health Promotion International, 2021. 36(6): p. 1578–1598.
Stokols, D. (1996). Translating social ecological theory into guidelines for community health promotion. American Journal of Health Promotion, 10(4), 282–298.
Bugeja, L., et al. (2014). Effectiveness of the 2005 compulsory personal flotation device (PFD) wearing regulations in reducing drowning deaths among recreational boaters in Victoria, Australia. Injury Prevention, 20(6), 387–392.
Cassell, E., & Newstead, S. (2015). Did compulsory wear regulations increase personal flotation device (PFD) use by boaters in small power recreational vessels? A before-after observational study conducted in Victoria, Australia. Injury Prevention, 21(1), 15–22.
Chung, C., et al. (2014). Informing policy on open water drowning prevention: an observational survey of life jacket use in Washington State. Injury Prevention, 20(4), 238–243.
Girasek, D. C. (2019). Evaluating a novel sign’s impact on whether park visitors enter a dangerous river. Injury Epidemiology, 6(1), 1–7.
Mangione, T., & Chow, W. (2014). Changing life jacket wearing behavior: an evaluation of two approaches. Journal of Public Health Policy, 35(2), 204–218.
Matthews, B., Andronaco, R., & Adams, A. (2014). Warning signs at beaches: do they work? Safety Science, 62, 312–318.
Moran, K. (2017). Rock-based fisher safety promotion: A decade on.International Journal of Aquatic Research and Education, 10(2).
Moran, K., Webber, J., & Stanley, T. (2017). The 4Rs of aquatic rescue: educating the public about safety and risks of bystander rescue. International Journal of Injury Control and Safety Promotion, 24(3), 396–405.
Petrass, L. A., & Blitvich, J. D. (2018). A lack of aquatic rescue competency: a drowning risk factor for young adults involved in aquatic emergencies. Journal of Community Health, 43(4), 688–693.
Quan, L., et al. (2021). Association of designated open water swim area regulations and open water drowning rates. Injury Prevention, 27(1), 10–16.
Savage, M. A., & Franklin, R. C. (2015). Exploring the delivery of swimming and water safety teacher training to culturally and linguistically diverse communities. International Journal of Aquatic Research and Education, 9(3), 241–256.
Schwebel, D. C., et al. (2011). The influence of simulated drowning audits on lifeguard surveillance and swimmer risk-taking at public swimming pools. International Journal of Aquatic Research and Education, 5(2), 210–218.
Scurati, R., et al. (2019). Towards a safe aquatic literacy: Teaching the breaststroke swimming with mobile devices’ support: a preliminary study. Journal of Physical Education and Sport, 19, 1999–2004.
Stempski, S., et al. (2015). Everyone swims: a community partnership and policy approach to address health disparities in drowning and obesity. Health Education & Behavior, 42(1S), 106S–114S.
Warton, N. M., & Brander, R. W. (2017). Improving tourist beach safety awareness: the benefits of watching Bondi Rescue. Tourism Management, 63, 187–200.
Willcox-Pidgeon, S. M., et al. (2021). Reducing inequities among adult female migrants at higher risk for drowning in Australia: the value of swimming and water safety programs. Health Promotion Journal of Australia, 32(S1), 49–60.
Artiga, E. A. Jr., et al. (2020). Effects of “Langoy sa Kaluwasan-Learn to Swim” extension project to the swimming competency of barangay emergency response personnel. International Journal of Human Movement and Sports Sciences, 8(6), 438–443.
Davoudi-Kiakalayeh, A. (2013). Evaluation of a community-based drowning prevention programme in northern Islamic Republic of Iran.Eastern Mediterranean Health Journal, 19(7).
Davoudi-Kiakalayeh, A., Mohammadi, R., & Yousefzadeh-Chabok, S. (2012). Prevention of drowning by community-based intervention: implications for low- and middle-income countries. Archives of Trauma Research, 1(3), 112–117.
Sansiritaweesook, G., & Kanato, M. (2015). Development of the model for local drowning surveillance system in northeastern Thailand. Journal of the Medical Association of Thailand = Chotmaihet Thangphaet, 98, S1–9.
Sansiritaweesook, G., et al. (2015). Effectiveness of community participation in a surveillance system initiative to prevent drowning in Thailand. Asia Pacific Journal of Public Health, 27(2), NP2677–NP2689.
Torlakovic, A., & Kebat, R. (2015). Efficiency of the training programme for non-swimmers adapted for women with a pronounced fear of being in water. Homo Sporticus, 1, 21–26.
Glanz, K., Rimer, B. K., & Viswanath, K. (2015). Health behavior: theory, research, and practice. Fifth edition. ed. Jossey-Bass Public Health. San Francisco, California: Jossey-Bass.
Cummings, P., Mueller, B., & Quan, L. (2011). Association between wearing a personal floatation device and death by drowning among recreational boaters: a matched cohort analysis of United States Coast Guard data. Injury Prevention, 17(3), 156–159.
Wold, B., & Mittelmark, M. B. (2018). Health-promotion research over three decades: the social-ecological model and challenges in implementation of interventions. Scandinavian Journal of Public Health, 46(20_suppl), 20–26.
Dawkins-Moultin, L., McDonald, A., & McKyer, L. (2016). Integrating the principles of socioecology and critical pedagogy for Health Promotion Health literacy interventions. Journal of Health Communication, 21(sup2), 30–35.
Golden, S. D., & Earp, J. A. L. (2012). Social Ecological Approaches to individuals and their contexts: twenty years of Health Education & Behavior Health Promotion Interventions. Health Education & Behavior, 39(3), 364–372.
Barnsley, P. D., Peden, A. E., & Scarr, J. (2018). Calculating the economic burden of fatal drowning in Australia. Journal of Safety Research, 67, 57–63.
Vlachantoni, I. T., Ntinapogias, A., & Petridou, E. (2013). Implementation of effective policies for the prevention of unintentional injuries: a feasibility study in european countries. Journal of Public Health, 21(1), 97–107.
Salmon, J. (2020). Changing Behavior using ecological models. The handbook of Behavior Change (p. 237). Cambridge: Cambridge University Press. L.D.C. M. S. Hagger, K. Hamilton, and T.L. N. Hankonen, Editors.
Birch, R. (2022). Rock fisher behaviours and perceptions regarding drowning risk assessed by direct observation and self-report: a public awareness campaign evaluation.Health Promotion Journal of Australia,
Glanz, K. (1997). Theory at a glance: a guide for health promotion practice. US Department of Health and Human Services, Public Health Service, National Institutes of Health.
Rosenstock, I. M. (2000). Health Belief Model. Kazdin, Alan E. (Ed). Encyclopedia of psychology. Oxford University Press. p. 78–80.
Ajzen, I. (2011). The theory of planned behaviour: reactions and reflections (pp. 1113–1127). Taylor & Francis.
Bunnell, R., et al. (2012). Fifty communities putting prevention to work: accelerating chronic disease prevention through policy, systems and environmental change. Journal of Community Health, 37(5), 1081–1090.
Green, L. W. (2022). A Model for Population Health Planning, Implementation, and Evaluation. Health Program Planning, Implementation, and Evaluation: Creating Behavioral, Environmental, and Policy Change, : p. 1.
Bauman, A., & Nutbeam, D. (2013). Evaluation in a nutshell: a practical guide to the evaluation of Health Promotion Programs. North Ryde, Australia: McGraw-Hill Education (Australia) Pty Limited.
Hyder, A. A., et al. (2014). A framework for addressing implementation gap in global drowning prevention interventions: experiences from Bangladesh. Journal of Health Population and Nutrition, 32(4), 564.
World Health Organization. (2017). Preventing drowning: an implementation guide. Geneva.
Koon, W., et al. (2021). Coastal drowning: a scoping review of burden, risk factors, and prevention strategies. PLoS One, 16(2), e0246034.
Scarr, J. P., et al. (2022). Tracing the emergence of drowning prevention on the global health and development agenda: a policy analysis. The Lancet Global Health, 10(7), e1058–e1066.
Scarr, J. P., & Jagnoor, J. (2022). Identifying opportunities for multisectoral action for drowning prevention: a scoping review.Injury Prevention,
Carman, J. G. (2007). Evaluation practice among community-based Organizations: Research into the reality. The American Journal of Evaluation, 28(1), 60–75.
Acknowledgements
Aleena Varghese Curtin University Master of Public Health student and Tanikka Gravatt, Bachelor of Science (Health Promotion) student for their contribution to data extraction and data synthesis.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
JEL and GC conceived the study design. Material preparation, data collection and analysis were performed by JEL, GC, CG, MDB and ND. Additional data analysis was performed by CG. The first draft of the manuscript was written by JEL and CG and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethics Approval
Not required as this is publicly available data.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Leavy, J.E., Gray, C., Della Bona, M. et al. A Review of Interventions for Drowning Prevention Among Adults. J Community Health 48, 539–556 (2023). https://doi.org/10.1007/s10900-023-01189-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-023-01189-6