
Abstract
Purpose
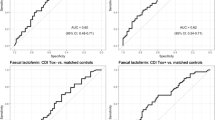
We investigated the role of fecal calprotectin (FC) and lactoferrin (FL) as predictive biomarkers in Clostridioides difficile infection (CDI).
Methods
We assembled a prospective cohort including all patients with a laboratory-confirmed CDI diagnosis between January and December 2017. FL and FC levels were measured at diagnosis by commercial ELISA and EIA kits. We investigated the diagnostic accuracy of FC and FL to predict CDI recurrence and severity (study outcomes) and explored optimal cut-off values in addition to those proposed by the manufacturers (200 µg/g and 7.2 µg/mL, respectively).
Results
We included 170 CDI cases (152 first episodes and 18 recurrences). The rates of recurrence (first episodes only) and severity (entire cohort) were 9.2% (14/152) and 46.5% (79/170). Both FL and FC levels were significantly higher in patients who developed study outcomes. Optimal cut-off values for FC and FL to predict CDI recurrence were 1052 µg/g and 6.0 µg/mL. The optimal cut-off value for FC yielded higher specificity (60.9%) and positive predictive value (PPV) (16.9%) than that proposed by the manufacturer. Regarding CDI severity, the optimal cut-off value for FC (439 µg/g) also provided higher specificity (43.9%) and PPV (54.1%) than that of the manufacturer, whereas the optimal cut-off value for FL (4.6 µg/mL) resulted in an improvement of PPV (57.5%).
Conclusion
By modifying the thresholds for assay positivity, the measurement of FC and FL at diagnosis is useful to predict recurrence and severity in CDI. Adding these biomarkers to current clinical scores may help to individualize CDI management.


Similar content being viewed by others


Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- aOR:
-
Adjusted odds ratio
- auROC:
-
Area under the receiver operator characteristic curve
- CCI:
-
Charlson comorbidity index
- CDI:
-
Clostridioides difficile Infection
- CI:
-
Confidence interval
- ED:
-
Emergency department
- EIA:
-
Enzyme immunoassay
- ELISA:
-
Enzyme-linked immunosorbent assay
- FDA:
-
Food and Drug Administration
- GDH:
-
Glutamate dehydrogenase
- HCFA:
-
Healthcare facility–associated
- IBD:
-
Inflammatory bowel disease
- IQR:
-
Interquartile range
- IV:
-
Intravenous
- NNAT:
-
Nucleic acid amplification testing
- NPV:
-
Negative predictive value
- PPI:
-
Proton-pump inhibitors
- PPV:
-
Positive predictive value
- SD:
-
Standard deviation
- SOT:
-
Solid organ transplantation
- WBC:
-
White blood cell count
References
Schaffler H, Breitruck A (2018) Clostridium difficile - from colonization to infection. Front Microbiol 9:646
Moore SC (2018) Clostridium difficile: more challenging than ever. Crit Care Nurs Clin North Am 30(1):41–53
Bouza E, Cobo J, Almirante B, Grupo de Trabajo C (2019) Recommendations from a panel of experts on the usefulness of fidaxomicin for the treatment of infections caused by Clostridium difficile. Rev Esp Quimioter 32(1):50–9
Song JH, Kim YS (2019) Recurrent Clostridium difficile infection: risk factors, treatment, and prevention. Gut Liver 13(1):16–24
Esteban-Vasallo MD, de Miguel-Diez J, Lopez-de-Andres A, Hernandez-Barrera V, Jimenez-Garcia R (2019) Clostridium difficile-related hospitalizations and risk factors for in-hospital mortality in Spain between 2001 and 2015. J Hosp Infect 102(2):148–156
Kelly CP (2012) Can we identify patients at high risk of recurrent Clostridium difficile infection? Clin Microbiol Infect 18(Suppl 6):21–27
Barbut F, Richard A, Hamadi K, Chomette V, Burghoffer B, Petit JC (2000) Epidemiology of recurrences or reinfections of Clostridium difficile-associated diarrhea. J Clin Microbiol 38(6):2386–2388
Johnson S, Lavergne V, Skinner AM et al (2021) Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults. Clin Infect Dis 73(5):755–757
van Prehn J, Reigadas E, Vogelzang EH et al (2021) European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect 27(Suppl 2):S1–S21
Reigadas E, van Prehn J, Falcone M et al (2021) How to: prophylactic interventions for prevention of Clostridioides difficile infection. Clin Microbiol Infect 27(12):1777–1783
Barbut F, Gouot C, Lapidus N et al (2017) Faecal lactoferrin and calprotectin in patients with Clostridium difficile infection: a case-control study. Eur J Clin Microbiol Infect Dis 36(12):2423–2430
Abou Chakra CN, Pepin J, Valiquette L (2012) Prediction tools for unfavourable outcomes in Clostridium difficile infection: a systematic review. PLoS ONE 7(1):e30258
Gallo A, Vallone C, Sabatelli L et al (2018) Fecal calprotectin in management of Clostridium difficile infection: a longitudinal study. Scand J Gastroenterol 53(5):567–572
Kim J, Kim H, Oh HJ et al (2017) Fecal calprotectin level reflects the severity of Clostridium difficile infection. Ann Lab Med 37(1):53–57
Boone JH, DiPersio JR, Tan MJ et al (2013) Elevated lactoferrin is associated with moderate to severe Clostridium difficile disease, stool toxin, and 027 infection. Eur J Clin Microbiol Infect Dis 32(12):1517–1523
Wen BJ, Te LG, Liu XX, Zhao JH (2022) The value of fecal calprotectin in Clostridioides difficile infection: a systematic review. Front Physiol 13:881816
Origuen J, Corbella L, Orellana MA et al (2018) Comparison of the clinical course of Clostridium difficile infection in glutamate dehydrogenase-positive toxin-negative patients diagnosed by PCR to those with a positive toxin test. Clin Microbiol Infect 24(4):414–421
Origuen J, Orellana MA, Fernandez-Ruiz M et al (2019) Toxin B PCR amplification cycle threshold adds little to clinical variables for predicting outcomes in Clostridium difficile infection: a retrospective cohort study. J Clin Microbiol 57(2):e01125-18
Bagdasarian N, Rao K, Malani PN (2015) Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA 313(4):398–408
McDonald LC, Gerding DN, Johnson S et al (2018) Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 66(7):987–994
Cohen SH, Gerding DN, Johnson S et al (2010) Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol 31(5):431–455
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383
Orellana-Miguel MA, Alcolea-Medina A, Barrado-Blanco L, Rodriguez-Otero J, Chaves-Sanchez F (2013) Algorithm proposal based on the C. Diff Quik Chek Complete ICT device for detecting Clostridium difficile infection. Enferm Infecc Microbiol Clin 31(2):97–99
Youden WJ (1950) Index for rating diagnostic tests. Cancer 3(1):32–35
Brandtzaeg P, Gabrielsen TO, Dale I, Muller F, Steinbakk M, Fagerhol MK (1995) The leucocyte protein L1 (calprotectin): a putative nonspecific defence factor at epithelial surfaces. Adv Exp Med Biol 371A:201–206
Sanchez L, Calvo M, Brock JH (1992) Biological role of lactoferrin. Arch Dis Child 67(5):657–661
Zar FA, Bakkanagari SR, Moorthi KM, Davis MB (2007) A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis 45(3):302–307
Perry DA, Shirley D, Micic D et al (2022) External validation and comparison of Clostridioides difficile severity scoring systems. Clin Infect Dis 74(11):2028–2035
Swale A, Miyajima F, Roberts P et al (2014) Calprotectin and lactoferrin faecal levels in patients with Clostridium difficile infection (CDI): a prospective cohort study. PLoS ONE 9(8):e106118
Suarez-Carantona C, Rodriguez-Torres A, Viteri-Noel A et al (2021) Usefulness of fecal calprotectin in the management of patients with toxigenic Clostridioides difficile. J Clin Med 10(8):1627
Rao K, Malani PN (2020) Diagnosis and treatment of Clostridioides (Clostridium) difficile infection in adults in 2020. JAMA 323(14):1403–1404
Ofori E, Ramai D, Dhawan M, Mustafa F, Gasperino J, Reddy M (2018) Community-acquired Clostridium difficile: epidemiology, ribotype, risk factors, hospital and intensive care unit outcomes, and current and emerging therapies. J Hosp Infect 99(4):436–442
Ooijevaar RE, van Beurden YH, Terveer EM et al (2018) Update of treatment algorithms for Clostridium difficile infection. Clin Microbiol Infect 24(5):452–462
El Feghaly RE, Stauber JL, Deych E, Gonzalez C, Tarr PI, Haslam DB (2013) Markers of intestinal inflammation, not bacterial burden, correlate with clinical outcomes in Clostridium difficile infection. Clin Infect Dis 56(12):1713–1721
Gateau C, Couturier J, Coia J, Barbut F (2018) How to: diagnose infection caused by Clostridium difficile. Clin Microbiol Infect 24(5):463–468
LaSala PR, Ekhmimi T, Hill AK, Farooqi I, Perrotta PL (2013) Quantitative fecal lactoferrin in toxin-positive and toxin-negative Clostridium difficile specimens. J Clin Microbiol 51(1):311–313
Wilcox MH, Gerding DN, Poxton IR et al (2017) Bezlotoxumab for prevention of recurrent Clostridium difficile infection. N Engl J Med 376(4):305–317
van Nood E, Vrieze A, Nieuwdorp M et al (2013) Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 368(5):407–415
Pawlowski SW, Warren CA, Guerrant R (2009) Diagnosis and treatment of acute or persistent diarrhea. Gastroenterology 136(6):1874–1886
Nicholson MR, Crews JD, Starke JR, Jiang ZD, DuPont H, Edwards K (2017) Recurrent Clostridium difficile infection in children: patient risk factors and markers of intestinal inflammation. Pediatr Infect Dis J 36(4):379–383
Funding
This study has been funded by an unrestricted grant from Merck Sharp & Dohme (MSD) and by Instituto de Salud Carlos III (ISCIII)—co-funded by the European Regional Development Fund / European Social Fund “A way to make Europe / Investing in your future”). M.F.R. holds a research contract “Miguel Servet” (CP18/00073) from the ISCIII, Spanish Ministry of Science and Innovation, also co-funded by the European Union. Funding sources had no involvement in the study design and conduction, data analysis, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
M. Á. participated in the study concept and design, data collection, and manuscript writing, drafting, and reviewing. J. O. participated in the clinical management of patients, study concept and design, data collection, and manuscript editing and reviewing. I. R.-G., R. S. J., and F. L.-M. participated in the clinical management of patients and manuscript editing and reviewing. P. P., T. R.-M., N. R., and M. Á. O. participated in the laboratory procedures and manuscript editing and reviewing. J. M. A. participated in the study concept and design, and manuscript editing and reviewing. M. F.-R. participated in the study concept and design, data analysis and interpretation, and manuscript writing, editing, and reviewing. All authors have read and approved the submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was submitted for evaluation and approved by the Ethics and Clinical Research Committee (CEIC) of the Research Institute Hospital “12 de Octubre” (i + 12). Informed consent was signed by all participants before inclusion in the study. All information related to the study was treated as strictly confidential in accordance with Organic Law 3/2018, of December 5, on Personal Data Protection and Guarantee of Digital Rights and the Biomedical Research Law 14/2007. The study was performed in accordance with the ethical principles set out in the latest version of the Helsinki
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ágreda Fernández, M., Origüen, J., Rodriguez-Goncer, I. et al. Predictive value of fecal calprotectin and lactoferrin levels for negative outcomes in Clostridioides difficile infection. Eur J Clin Microbiol Infect Dis 43, 313–324 (2024). https://doi.org/10.1007/s10096-023-04729-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-023-04729-z