
Abstract
Background
Prophylactic mesh augmentation in emergency laparotomy closure is controversial. We aimed to perform a meta-analysis of randomized controlled trials (RCT) evaluating the placement of prophylactic mesh during emergency laparotomy.
Methods
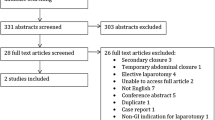
We performed a systematic review of Cochrane, Scopus, and PubMed databases to identify RCT comparing prophylactic mesh augmentation and no mesh augmentation in patients undergoing emergency laparotomy. We excluded observational studies, conference abstracts, elective surgeries, overlapping populations, and trial protocols. Postoperative outcomes were assessed by pooled analysis and meta-analysis. Statistical analysis was performed using RevMan 5.4. Heterogeneity was assessed with I2 statistics. Risk of bias was assessed using the revised Cochrane risk-of-bias tool (RoB 2). The review protocol was registered at PROSPERO (CRD42023412934).
Results
We screened 1312 studies and 33 were thoroughly reviewed. Four studies comprising 464 patients were included in the analysis. Mesh reinforcement was significantly associated with a decrease in incisional hernia incidence (OR 0.18; 95% CI 0.07–0.44; p < 0.001; I2 = 0%), and synthetic mesh placement reduced fascial dehiscence (OR 0.07; 95% CI 0.01–0.53; p = 0.01; I2 = 0%). Mesh augmentation was associated with an increase in operative time (MD 32.09 min; 95% CI 6.39–57.78; p = 0.01; I2 = 49%) and seroma (OR 3.89; 95% CI 1.54–9.84; p = 0.004; I2 = 0%), but there was no difference in surgical-site infection or surgical-site occurrences requiring procedural intervention or reoperation.
Conclusions
Mesh augmentation in emergency laparotomy decreases incisional hernia and fascial dehiscence incidence. Despite the risk of seroma, prophylactic mesh augmentation appears to be safe and might be considered for emergency laparotomy closure. Further studies evaluating long-term outcomes are still needed.











Similar content being viewed by others


Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
References
Ahmed J, Hasnain N, Fatima I et al (2020) Prophylactic mesh placement for the prevention of incisional hernia in high-risk patients after abdominal surgery: a systematic review and meta-analysis. Cureus 12:e10491
Deerenberg EB, Harlaar JJ, Steyerberg EW et al (2015) Small bites versus large bites for closure of abdominal midline incisions (STITCH): a double-blind, multicentre, randomised controlled trial. The Lancet 386:1254–1260
Deerenberg EB, Henriksen NA, Antoniou GA et al (2022) Updated guideline for closure of abdominal wall incisions from the European and American Hernia Societies. Br J Surg 109:1239–1250
Luijendijk RW, Hop WCJ, van den Tol MP et al (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–398
Kenig J, Richter P, Żurawska S et al (2012) Risk factors for wound dehiscence after laparotomy - clinical control trial. Pol Przegl Chir 84:565–573
Albendary M, Mohamedahmed AYY, Alamin A et al (2022) Efficacy and safety of mesh closure in preventing wound failure following emergency laparotomy: a systematic review and meta-analysis. Langenbecks Arch Surg 407:1333–1344
Ulutas ME, Sahin A, Simsek G, et al (2023) Does onlay mesh placement in emergency laparotomy prevent incisional hernia? A prospective randomized double-blind study. Hernia J Hernias Abdom Wall Surg
Pizza F, D’Antonio D, Ronchi A et al (2021) Prophylactic sublay non-absorbable mesh positioning following midline laparotomy in a clean-contaminated field: randomized clinical trial (PROMETHEUS). Br J Surg 108:638–643
Haskins IN, Horne CM, Krpata DM et al (2018) A call for standardization of wound events reporting following ventral hernia repair. Hernia 22:729–736
Higgins JPT, Altman DG, Gotzsche PC et al (2011) The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928–d5928
McGuinness LA, Higgins JPT (2020) Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods n/a
Page MJ, McKenzie JE, Bossuyt PM, et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ n71
Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C (2017) User manual for trial sequential analysis (TSA), 2nd ed. Copenhagen: Copenhagen Trial Unit, pp 1–119. https://ctu.dk/tsa/. Accessed 21 Aug 2023
Jakobsen JC, Wetterslev J, Winkel P et al (2014) Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods. BMC Med Res Methodol 14:120. https://doi.org/10.1186/1471-2288-14-120
Balshem H, Helfand M, Schünemann HJ et al (2011) GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 64:401–406
Jakob M, Haltmeier T, Candinas D, Beldi G (2020) Biologic mesh implantation is associated with serious abdominal wall complications in patients undergoing emergency abdominal surgery: a randomized-controlled clinical trial. J Trauma Acute Care Surg 89:1149–1155
Lima H, Rasslan R, Novo F et al (2020) Prevention of fascial dehiscence with onlay prophylactic mesh in emergency laparotomy: a randomized clinical trial. J Am Coll Surg 230:76–87
Chapter 13: Assessing risk of bias due to missing results in a synthesis. https://training.cochrane.org/handbook/current/chapter-13. Accessed 19 Aug 2023
Moussavian MR, Schuld J, Dauer D et al (2010) Long term follow up for incisional hernia after severe secondary peritonitis—incidence and risk factors. Am J Surg 200:229–234
Olavarria OA, Dhanani NH, Bernardi K et al (2023) Prophylactic mesh reinforcement for prevention of midline incisional hernias: a publication bias adjusted meta-analysis. Ann Surg 277:E162–E169
Alsaadi D, Stephens I, Simmons LO et al (2022) Prophylactic onlay mesh at emergency laparotomy: promising early outcomes with long-acting synthetic resorbable mesh. Anz J Surg 92:2218–2223
Mehdorn M, Groos L, Kassahun W et al (2021) Interrupted sutures prevent recurrent abdominal fascial dehiscence: a comparative retrospective single center cohort analysis of risk factors of burst abdomen and its recurrence as well as surgical repair techniques. BMC Surg 21:208
van Ramshorst GH, Nieuwenhuizen J, Hop WCJ et al (2010) Abdominal wound dehiscence in adults: development and validation of a risk model. World J Surg 34:20–27
van Ramshorst GH, Eker HH, van der Voet JA et al (2013) Long-term outcome study in patients with abdominal wound dehiscence: a comparative study on quality of life, body image, and incisional hernia. J Gastrointest Surg 17:1477–1484
Poli M, de Figueiredo S, Tastaldi L, Mao R-MD et al (2023) Biologic versus synthetic mesh in open ventral hernia repair: a systematic review and meta-analysis of randomized controlled trials. Surgery S0039–6060(22):01030–01033
Höer J, Lawong G, Klinge U, Schumpelick V (2002) Factors influencing the development of incisional hernia. A retrospective study of 2983 laparotomy patients over a period of 10 years. Chir Z Alle Geb Oper Medizen 73:474–480
Sørensen LT, Hemmingsen U, Kallehave F et al (2005) Risk factors for tissue and wound complications in gastrointestinal surgery. Ann Surg 241:654–658
Majumder A, Winder JS, Wen Y et al (2016) Comparative analysis of biologic versus synthetic mesh outcomes in contaminated hernia repairs. Surgery 160:828–838
Pereira-Rodríguez JA, Amador-Gil S, Bravo-Salva A et al (2022) Implementing a protocol to prevent incisional hernia in high-risk patients: a mesh is a powerful tool. Hernia 26:457–466
Sanchez VM, Abi-Haidar YE, Itani KMF (2011) Mesh infection in ventral incisional hernia repair: incidence, contributing factors, and treatment. Surg Infect 12:205–210
Birolini C, de Miranda JS, Tanaka EY et al (2020) The use of synthetic mesh in contaminated and infected abdominal wall repairs: challenging the dogma—a long-term prospective clinical trial. Hernia 24:307–323
Choi JJ, Palaniappa NC, Dallas KB et al (2012) Use of mesh during ventral hernia repair in clean-contaminated and contaminated cases: outcomes of 33,832 cases. Ann Surg 255:176–180
Holihan JL, Nguyen DH, Nguyen MT et al (2016) Mesh location in open ventral hernia repair: a systematic review and network meta-analysis. World J Surg 40:89–99
Jairam A, Timmermans L, Eker H et al (2017) Prevention of incisional hernia with prophylactic onlay and sublay mesh reinforcement versus primary suture only in midline laparotomies (PRIMA): 2-year follow-up of a multicentre, double-blind, randomised controlled trial. Lancet Lond Engl 390:567–576
Montelione KC, Zolin SJ, Fafaj A et al (2021) Outcomes of redo-transversus abdominis release for abdominal wall reconstruction. Hernia 25:1581–1592
Holland AJA, Castleden WM, Norman PE, Stacey MC (1996) Incisional hernias are more common in aneurysmal arterial disease. Eur J Vasc Endovasc Surg 12:196–200
Antoniou GA, Giannoukas AD, Georgiadis GS et al (2011) Increased prevalence of abdominal aortic aneurysm in patients undergoing inguinal hernia repair compared with patients without hernia receiving aneurysm screening. J Vasc Surg 53:1184–1188
Curro G, Centorrino T, Low V et al (2012) Long-term outcome with the prophylactic use of polypropylene mesh in morbidly obese patients undergoing biliopancreatic diversion. Obes Surg 22:279–282
Xing L, Culbertson EJ, Wen Y et al (2011) Impaired laparotomy wound healing in obese rats. Obes Surg 21:1937–1946
Sun M, Xu M, Sun J (2023) Risk factor analysis of postoperative complications in patients undergoing emergency abdominal surgery. Heliyon 9:e13971
Tolstrup M-B, Watt SK, Gögenur I (2017) Morbidity and mortality rates after emergency abdominal surgery: an analysis of 4346 patients scheduled for emergency laparotomy or laparoscopy. Langenbecks Arch Surg 402:615–623
San Miguel C, Melero D, Jiménez E et al (2018) Long-term outcomes after prophylactic use of onlay mesh in midline laparotomy. Hernia 22:1113–1122
Sørensen LT (2005) Smoking is a risk factor for incisional hernia. Arch Surg 140:119
Franchi M (2001) Incisional hernia in gynecologic oncology patients: a 10-year study. Obstet Gynecol 97:696–700
Timmermans L, de Goede B, Eker HH et al (2013) Meta-analysis of primary mesh augmentation as prophylactic measure to prevent incisional hernia. Dig Surg 30:401–409
Fischer JP, Basta MN, Wink JD et al (2015) Cost-utility analysis of the use of prophylactic mesh augmentation compared with primary fascial suture repair in patients at high risk for incisional hernia. Surgery 158:700–711
Funding
No funding was received for this work.
Author information
Authors and Affiliations
Contributions
SMPF conceived the idea and study design. PM, BOT and SBM participated in the data collection and analysis. All authors participated in the data interpretation, writing and critical revision of the work.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interest.
Ethical approval
Due to the nature of this study, it is exempt from the requirement for ethical board registration and individual patient consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Marcolin, P., Mazzola Poli de Figueiredo, S., Oliveira Trindade, B. et al. Prophylactic mesh augmentation in emergency laparotomy closure: a meta-analysis of randomized controlled trials with trial sequential analysis. Hernia (2024). https://doi.org/10.1007/s10029-023-02943-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10029-023-02943-4