
Abstract
Aims/hypothesis
Fatty acid-binding protein 4 (FABP4) is an adipokine with a key regulatory role in glucose and lipid metabolism. We prospectively evaluated the role of FABP4 in the pathophysiology of diabetic ketoacidosis (DKA) in new-onset type 1 diabetes.
Methods
Clinical and laboratory data were prospectively collected from consecutive children presenting with new-onset type 1 diabetes. In addition to blood chemistry and gases, insulin, C-peptide, serum FABP4 and NEFA were collected upon presentation and 48 h after initiation of insulin treatment. In a mouse model of type 1 diabetes, glucose, insulin, β-hydroxybutyrate and weight were compared between FABP4 knockout (Fabp4−/−) and wild-type (WT) mice.
Results
Included were 33 children (mean age 9.3 ± 3.5 years, 52% male), of whom 14 (42%) presented with DKA. FABP4 levels were higher in the DKA group compared with the non-DKA group (median [IQR] 10.1 [7.9–14.2] ng/ml vs 6.3 [3.9–7] ng/ml, respectively; p = 0.005). The FABP4 level was positively correlated with HbA1c at presentation and inversely correlated with venous blood pH and bicarbonate levels (p < 0.05 for all). Following initiation of insulin therapy, a marked reduction in FABP4 was observed in all children. An FABP4 level of 7.22 ng/ml had a sensitivity of 86% and a specificity of 78% for the diagnosis of DKA, with an area under the receiver operating characteristic curve of 0.78 (95% CI 0.6, 0.95; p = 0.008). In a streptozotocin-induced diabetes mouse model, Fabp4−/− mice exhibited marked hypoinsulinaemia and hyperglycaemia similar to WT mice but displayed no significant increase in β-hydroxybutyrate and were protected from ketoacidosis.
Conclusions/interpretation
FABP4 is suggested to be a necessary regulator of ketogenesis in insulin-deficient states.
Graphical abstract

Similar content being viewed by others


Introduction
Fatty acid-binding proteins are a family of intracellular lipid chaperones that were identified as critical molecules responsible for the integration of intracellular signalling and metabolic stress and regulation [1, 2]. Fatty acid-binding protein 4 (FABP4), also known as aP2, is an adipokine, the secretion of which is enhanced under lipolytic stimuli and is inhibited by insulin [3, 4]. Adipocyte-derived FABP4 promotes hepatic glucose production during fasting [5], and Fabp4 deletion in mice is sufficient to protect the mice from insulin resistance and diabetes [6]. In humans, circulating FABP4 levels have been linked to obesity, type 2 diabetes and atherosclerosis and to poor glycaemic control in type 1 diabetes [7,8,9,10]. Additionally, another study demonstrated that serum FABP4 may serve as a biomarker for prediction of pre-eclampsia in pregnant women with type 1 diabetes [11].
Type 1 diabetes is one of the most common chronic diseases in childhood. The incidence of type 1 diabetes among children and adolescents increases every year at a rate of 3–15% worldwide [12,13,14]. Up to 80% of children with newly diagnosed type 1 diabetes present with diabetic ketoacidosis (DKA) [15], which is the most common cause of hospitalisation, cerebral oedema and death among children with type 1 diabetes [16, 17].
Upon presentation, individuals with type 1 diabetes exhibit complex metabolic alterations of cellular starvation and dehydration, enhanced lipolysis and ketogenesis, and marked hyperglycaemia. This may lead to a life-threatening DKA. Since FABP4 is an adipokine with key hormonal functions in systemic glucose and lipid metabolism, we aimed to determine the importance of FABP4 in new-onset type 1 diabetes, before initiation of insulin therapy.
Methods
Study design
Clinical and laboratory data were prospectively collected from children who presented with new-onset type 1 diabetes to a single tertiary medical centre. The clinical data included age at diagnosis, sex, anthropometric measurements and Tanner stage. Inclusion criteria were children between the ages of 6 months and 18 years with new-onset type 1 diabetes. The participants were divided into DKA and non-DKA groups, and into prepubertal children and pubertal adolescents.
The criteria for diagnosis of DKA were venous blood pH <7.3 and/or HCO3−<15 mmol/l with evidence of ketones [18]. The parents gave informed consent, and the assent was sought and obtained from the children involved in this study. The Institutional Review Board of Sheba Medical Center approved the study protocol (protocol ID: 2108–15-SMC).
Anthropometric measurements
Anthropometric data comprised of weight, height and BMI. Standing height was measured to the nearest 0.1 cm using a wall-mounted stadiometer, and body weight was obtained to the nearest 0.1 kg. BMI was calculated based on the formula weight (kg)/height (m)2. Height, weight and BMI SD scores were calculated using age and sex-specific growth data (based on the US Center for Disease Control and Prevention, Year 2000 Growth Charts, which were found to be appropriate also for Israeli children and youth [19]).
Laboratory assessment
Laboratory data for all participants included glucose, blood gases, anti-GAD antibody titre and HbA1c. The metabolic data added for this study consisted of serum levels of insulin, C-peptide, FABP4 and NEFA. FABP4 and NEFA were collected upon presentation and at 48 h after initiation of insulin treatment. FABP4 was measured using DuoSet ELISA (R&D Systems, Minneapolis, USA), and NEFA were measured using Quantification kit (Abcam, USA) according to the manufacturer instructions. Insulin and C-peptide were measured by Immulite 2000 (Siemens Medical Solutions Diagnostics, UK). HbA1c was measured by Variant II Turbo (Bio-Rad, California, USA), and anti-GAD was measured by RIA kit (RSR, UK). Serum glucose and serum gases were measured using Cobas b 211 (Roche Diagnostics, Rotkreuz, Switzerland).
Animals
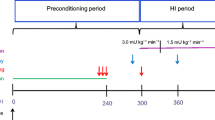
Insulin deficiency was induced by injecting 12-week-old C57BL/6 wild-type (WT) mice and Fabp4−/− mice (kindly provided by G. Hotamisligil, The Sabri Ülker Center, Harvard T.H. Chan School of Public Health, Boston, MA, USA) with streptozotocin (STZ) [20]. Mice were fed with regular chow diet. After mice were starved overnight, they were injected with 200 mg/kg STZ (Sigma-Aldrich, Israel S0130). STZ was dissolved in 0.1 mol/l citrate buffer pH 4.5. Mouse weight and glucose were monitored daily. Fat mass in mice of both groups was assessed using NMR spectroscopy at baseline. Glucose levels were determined from the tail vein using FreeStyle strips (Abbott, USA). Ketones (β-hydroxybutyrate [βOHB]) were measured with a ketometer (Abbott) before injection and daily from day 2 until the mice were killed by isoflurane inhalation on day 4. Insulin concentrations were determined in plasma samples using ELISA according to the manufacturer’s instructions (Ultrasensitive Mouse Insulin ELISA; Mercodia, Sweden), and NEFA were measured using Quantification kit (Abcam) according to the manufacturer’s instructions. Under anaesthesia, blood was taken from the vena cava using a gas syringe. We repeated this experiment four times with similar results. This part of the study was approved by the Institutional Animal Care and Use Committee (protocol ID: 1310/12/ANIM).
Statistical analysis
Statistical analysis was performed on IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., New York, USA, www.spss.com) and GraphPad Prism9 (GraphPad Software, USA, www.graphpad.com). Continuous variables are presented as mean ± SD and compared using Student’s t test. Abnormally distributed continuous variables are presented as medians and IQRs and compared using the Mann–Whitney test. Categorical variables were analysed using the χ2 test and presented as percentages. Correlations between continuous abnormally distributed variables were described using Spearman’s correlation test, and correlations between continuous normally distributed variables were assessed using Pearson’s correlation test. FABP4 distributed abnormally, therefore correlations between FAPB4 and each of the variables were assessed using the Spearman’s correlation test. NEFA distributed normally, therefore correlations between NEFA and normally distributed variables (weight SDS, BMI SDS and glucose) were conducted using the Pearson’s correlation test. Correlations between NEFA and abnormally distributed variables (pH, HCO3−, insulin, C-peptide, HbA1c, FABP4 and anti-GAD) were conducted using the Spearman’s correlation test.
The adjusted risk for DKA at presentation, defined as venous blood pH < 7.30, was assessed using multivariable logistic regression model, including the following variables: serum FABP4 levels, female sex, age, weight SDS, HbA1c, glucose, C-peptide levels and anti-GAD antibody titre. The analysis was performed using the enter method for variables inclusion. The OR and 95% CI for each variable were reported. FABP4 cut-off was determined using the receiver operating characteristic (ROC) curve analysis, and the AUC was calculated with 95% CIs. Continuous variables were used as dichotomous (below median vs at/above median), and FABP4 was used as dichotomous, based on the point of maximal sensitivity and specificity. A two-tailed p value of <0.05 was used for defining statistical significance.
Results
We enrolled 40 consecutive children presenting with new-onset type 1 diabetes into the study; seven children were excluded due to missing data. The remaining 33 eligible children had a mean age of 9.3 ± 3.5 years, 17 (52%) were male and 14 (42%) presented with DKA. There were no statistically significant differences in sex, age, weight, height, BMI SDS or puberty status between the DKA and non-DKA groups (Table 1). The C-peptide level was lower in the DKA vs non-DKA group (median [IQR] 0.3 [0.1–0.4] vs 0.4 [0.3–0.8] ng/ml, respectively; p = 0.03) (Table 1) and the serum FABP4 level was higher in the DKA vs non-DKA group (median [IQR] 10.1 [7.9–14.2] vs 6.3 [3.9–7] ng/ml, respectively; p = 0.005) (Fig. 1a and Table 1).

(a–c) Median (IQR) serum FABP4 levels in DKA and non-DKA groups at new-onset type 1 diabetes (a), at 48 h after commencing insulin (n = 14 in DKA group; n = 19 in non-DKA group) (b), and at new-onset type 1 diabetes among female and male participants (c). (d–n) Correlation analysis between serum FABP4 levels and weight SDS (d), height SDS (e), BMI SDS (f), serum glucose (g), serum insulin (h), serum NEFA (i), serum HbA1c (j), serum C-peptide levels (k), serum anti-GAD titre (l), serum pH (m) and serum HCO3− (n) in participants with new-onset type 1 diabetes. (o) ROC curve for the detection of pH < 7.3 by FABP4 levels in participants with new-onset type 1 diabetes (AUC = 0.78). **p < 0.01 for DKA vs non-DKA
Following initiation of insulin therapy, a marked reduction in serum FABP4 was observed in all of the participants (Fig. 1b). There was no difference between female and male participants in serum FABP4 level (p = 0.5, Fig. 1c), and no correlation was observed between FABP4 and anthropometric measurements (weight SDS, r = 0.17, p = 0.35; height SDS, r = 0.06, p = 0.71, BMI SDS, r = 0.27, p = 0.14; Fig. 1d–f). In addition, there was no significant correlation between FABP4 and glucose (r = 0.12, p = 0.5; Fig. 1g), insulin (r = −0.2, p = 0.31; Fig. 1h) or NEFA (r = 0.15, p = 0.21; Fig. 1i) level upon presentation to the emergency department. However, FABP4 positively correlated with HbA1c (r = 0.36, p = 0.04; Fig. 1j), negatively correlated with C-peptide level (r = −0.38, p = 0.06; Fig. 1k) and anti-GAD titre (r = −0.43, p = 0.01; Fig. 1l), and strongly and negatively correlated with blood pH (r = −0.53, p = 0.002; Fig. 1m) and HCO3− (r = −0.5, p = 0.001; Fig. 1n). Serum NEFA levels were correlated negatively with HCO3− (r = −0.43, p = 0.03) and pH, although the latter correlation did not reach statistical significance (r = −0.39, p = 0.059), but did not correlate with weight SDS, BMI SDS, HbA1c, insulin, C-peptide or anti-GAD. Lastly, a positive correlation was observed between the levels of FABP4 and NEFA only after insulin treatment has been initiated (r = 0.53, p = 0.007).
In an analysis of prepubertal vs pubertal patients, the median (IQR) FABP4 level at presentation was similar in the two groups: 6.9 (4.1–12.6) vs 8.1 (5.2–11.3) ng/ml; p = 0.89 (ESM Fig. 1). However, following initiation of insulin therapy serum FABP4 declined by 67% in the prepubertal group but only by 43% in the pubertal group (p < 0.0001 and p = 0.002, respectively; ESM Fig. 1).
In a ROC curve analysis, a cut-off value for FABP4 serum levels ≥7.22 ng/ml had a sensitivity of 86% and a specificity of 78% for detecting the presence of DKA, with an AUC of 0.78 (95% CI 0.6, 0.95, p = 0.008; Fig. 1o). In a multivariable logistic regression analysis, an FABP4 level ≥ 7.22 ng/ml, was the only variable independently associated with increased odds of DKA (OR 70.06 [95% CI 1.2, 4097.6], p = 0.04; Table 2).
To assess the potential mechanistic role for FABP4 in mediating ketogenesis, we injected FABP4 null (Fabp4−/−) mice and WT controls with STZ and monitored their blood glucose, βOHB, plasma insulin, and NEFA levels. STZ treatment resulted in a similar decrease in insulin levels in WT and Fabp4−/− mice (Fig. 2a) and a similar rise in blood glucose (Fig. 2b). Yet, while an expected rise in βOHB level was observed in WT mice 4 days post STZ injection (from 2.1 ± 1.2 mmol/l at baseline to 3.1 ± 1.4 mmol/l 4 days post STZ injection, p = 0.006), no significant change in βOHB was detected in Fabp4−/− mice (1.9 ± 0.4 to 1.6 ± 1.4 mmol/l, p = 0.1). When comparing the change in βOHB levels from baseline to 4 days after STZ treatment, a twofold difference was observed between WT and Fabp4−/− mice (p = 0.004, Fig. 2c). Plasma NEFA levels measured 4 days after STZ treatment were higher in WT compared with Fabp4−/− mice, although the difference did not reach statistical significance (p = 0.07, Fig. 2d). In addition, WT mice exhibited a marked hypoinsulinaemia-related catabolic state, with a body weight loss twice that of Fabp4−/− mice who were protected from a significant weight loss despite a significant hypoinsulinaemia and hyperglycaemia (10% vs 5%, respectively; p = 0.007) (Fig. 2e). It is important to add that the baseline weight of the mice in the two groups did not differ significantly (23.2 ± 1.7 g in WT mice vs 22.5 ± 2.1 g in Fabp4−/− mice; p = 0.19), nor did fat mass with 27.79 ± 2.2% fat observed in WT mice vs 26.32 ± 1.71% in Fabp4−/− mice (p = 0.13).

Mean ± SEM plasma insulin (a), blood glucose (b), blood βOHB (n = 23 in WT mice, n = 28 in Fabp4−/− mice) (c) and plasma NEFA (d) levels, and body weight (n = 22 in WT mice, n = 26 in Fabp4−/− mice) (e) in WT and Fabp4−/− mice in a mouse model of type 1 diabetes. Measurements were taken at baseline and up to day 4 post injection of STZ, which induced insulin-deficiency diabetes. *p < 0.05 and **p < 0.01 for Fabp4−/− vs WT mice
Discussion
The current study suggests FABP4 as a potential regulator of ketogenesis in the pathophysiology of DKA in both mice and humans. In humans, we showed that FABP4 is sensitive and specific for the detection of DKA, being superior to any other clinical variable. In addition, the rapid and marked reduction in FABP4 levels following insulin initiation further supports the tight regulation of FABP4 secretion by insulin [3, 7]. In mice, we demonstrated that in the absence of FABP4, insulin deficiency was unable to induce significant production of βOHB, supporting its direct role in the pathophysiology of DKA. Taken together, our data demonstrate that the adipokine FABP4 is necessary in mediating ketogenesis, even under extreme insulin-deficient conditions.
FABP4 has been demonstrated not only to tightly correlate with obesity and fat mass [21, 22] but also to act as a mediator of obesity-related metabolic abnormalities such as insulin resistance, diabetes and atherosclerosis [2]. Here we showed that in untreated type 1 diabetes, an extreme insulin-deficient state, FAPB4 level lost its association with both sex and anthropometric measures. Our observation in humans is in agreement with the findings of Cao et al. [7] demonstrating increased FABP4 levels during fasting, irrespective of fat mass. These and other studies have thus identified FABP4 as an adipokine that is tightly regulated by nutritional status and as an important component of the systemic adaptive response to fasting [5, 7]. Additional support for the mechanistic role of FABP4 in metabolic regulation during fasting comes from its stimulatory effects on hepatic glucose production [7] and glycogenolysis [23]. Our results add a further component by demonstrating FABP4’s potential role as a mediator of ketogenesis. The exact mechanism(s) by which FABP4 regulates ketogenesis cannot be elucidated in this clinical/translational study and may include the regulation of NEFA release from adipose tissue, hepatic delivery of NEFA and/or a direct effect on liver ketone synthesis. There is evidence to suggest that FABP4 may exert its pro-ketogenic effects by synergistically regulating both NEFA supply from the adipose tissue and utilisation in the liver. In fact, FABP4-deficient adipocytes have been demonstrated to exhibit reduced efficiency of basal and β-adrenergic stimulated lipolysis, both in-vivo and in-vitro [24, 25], thus attenuating hepatic delivery of NEFA in DKA. The greater reduction in body weight in WT mice and the higher levels of NEFA following STZ treatment, may suggest that decreased lipolysis in Fabp4−/− may be an important contributor. Yet, given the vast excess of NEFA under insulin-deficient conditions, the rate-controlling steps of ketogenesis are considered to be the mitochondrial transfer of NEFA via carnitine acyltransferase I and utilisation via 3-hydroxy-3-methylglutaryl-CoA synthase (HMGCS2) [26]. Of interest, FABP4 has been implicated in the regulation of genes encoding both of these, albeit this has not been assessed directly. Regardless of the exact mechanism of action of FABP4, its potential regulatory role in glycogenolysis, gluconeogenesis and ketogenesis highlights this adipokine as an important partner of glucagon in mediating its biological activities.
FABP4’s role in DKA pathophysiology reported here is supported by functional studies in mice. During nutrient deprivation, a primary function of adipose tissue is to augment lipolysis. Induction of lipolysis in mice resulted in a rapid increase in plasma FABP4 levels, further linking FABP4 secretion to lipolytic signals. Thus, the increase in FABP4 level during fasting likely represents increased adipocyte lipolytic activity [7]. In fact, Fabp4−/− mice exhibit a decreased lipolytic activity even under conditions known to stimulate lipolysis [27]. This corroborates with the reduced ketogenesis we observed in Fabp4−/− mice, which consequently lost less of their body weight after STZ injection. The enhanced lipolysis in type 1 diabetes likely contributes to the rise in both circulating FABP4 and NEFA levels, leading to the development of DKA, and both effectors are rapidly suppressed upon initiation of insulin therapy [28].
The incidence of DKA in our cohort is similar to that reported in a larger cohort from our centre, described in 2015 [29], as well as in reports from other countries [15, 30], highlighting the relatively high rate of DKA as a presenting metabolic emergency in new-onset type 1 diabetes in children. As such, better understanding of the metabolic regulation of excessive ketogenesis is important, especially among children at high risk for the development of type 1 diabetes. Here we demonstrate that FABP4 was superior to other metabolic variables such as NEFA, glucose, C-peptide or insulin as markers of DKA. This underlines the difference between FABP4 and NEFA despite their co-secretion from adipose tissue. Re-esterification, tissue uptake and efficient metabolism of NEFA may explain this apparent discrepancy, emphasising the potential utility of FABP4 as an integrative biomarker for the acute metabolic state of severe insulin deficiency.
In pubertal children, compared with prepubertal children, we observed that insulin treatment was less effective in decreasing FABP4 and NEFA levels. Notably, puberty is associated with a marked decrease in insulin sensitivity and a higher fat mass, which likely explains our observations [31]. In support is a study of 124 children aged 6–14 years old, in which FABP4 levels were positively correlated with pubertal stage [22].
Our study has several limitations. We did not have data on FABP4 levels once glucose levels and body weight have stabilised. Yet, the rapid decrease in FABP4 within only 2 days of insulin therapy argues against an inherent difference between the two groups (DKA and non-DKA). Similarly, we did not have any determinations of FABP4 levels prior to diagnosis of type 1 diabetes, which might have highlighted FABP4 as a reliable predictive biomarker for at-risk individuals during the prediabetic state. In addition, in this set of experiments we could not determine whether the marked inhibition of ketogenesis in the absence of FABP4 is due to inhibition of lipolysis at the level of the adipose tissue or a decrease in glucagon bioactivity in the liver. Yet, as discussed above, accumulating data demonstrating the role of FABP4 in both glycogenolysis and gluconeogenesis argue in favour of the latter as an important mechanism for the effects of FABP4.
In summary, we report that the adipokine FABP4 is increased in insulin deficiency and particularly in the setting of DKA among children with new-onset type 1 diabetes, and declines rapidly after commencement of insulin therapy. In a mouse model of type 1 diabetes, FABP4 deletion resulted in a marked reduction in ketogenesis. Our study suggests that circulating FABP4 may play a regulatory role in DKA pathogenesis and may serve as a biomarker for metabolic characterisation of deficient bioactivity of insulin. Since FABP4 is involved in both glucose and lipid metabolism, its circulating levels may be seen as an integration of insulin action at the level of the adipose tissue, with tight correlation to lipolysis, ketogenesis and hepatic glucose production. Therefore, FABP4 is an ideal readout of systemic metabolism in the setting of both insulin resistance and insulin deficiency.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Abbreviations
- DKA:
-
Diabetic ketoacidosis
- FABP4:
-
Fatty acid-binding protein 4
- βOHB:
-
β-Hydroxybutyrate
- ROC:
-
Receiver operating characteristic
- SDS:
-
SD score
- STZ:
-
Streptozotocin
- WT:
-
Wild-type
References
Furuhashi M, Hotamisligil GS (2008) Fatty acid-binding proteins: role in metabolic diseases and potential as drug targets. Nat Rev Drug Discov 7(6):489–503. https://doi.org/10.1038/nrd2589
Hotamisligil GS, Bernlohr DA (2015) Metabolic functions of FABPs - mechanisms and therapeutic implications. Nat Rev Endocrinol 11:592–605. https://doi.org/10.1038/nrendo.2015.122
Ertunc ME, Sikkeland J, Fenaroli F et al (2015) Secretion of fatty acid binding protein aP2 from adipocytes through a nonclassical pathway in response to adipocyte lipase activity. J Lipid Res 56(2):423–434. https://doi.org/10.1194/jlr.M055798
Mita T, Furuhashi M, Hiramitsu S et al (2015) FABP4 is secreted from adipocytes by adenyl cyclase-PKA- and guanylyl cyclase-PKG-dependent lipolytic mechanisms. Obesity (Silver Spring) 23(2):359–367. https://doi.org/10.1002/oby.20954
Syamsunarno MRAA, Iso T, Hanaoka H et al (2013) A critical role of fatty acid binding protein 4 and 5 (FABP4/5) in the systemic response to fasting. PLoS One 8(11):e79386. https://doi.org/10.1371/journal.pone.0079386
Hotamisligil GS, Johnson RS, Distel RJ, Ellis R, Papaioannou VE, Spiegelman BM (1996) Uncoupling of obesity from insulin resistance through a targeted mutation in aP2, the adipocyte fatty acid binding protein. Science 274(5291):1377–1379. https://doi.org/10.1126/science.274.5291.1377
Cao H, Sekiya M, Ertunc ME et al (2013) Adipocyte lipid chaperone AP2 is a secreted adipokine regulating hepatic glucose production. Cell Metab 17(5):768–778. https://doi.org/10.1016/j.cmet.2013.04.012
Kralisch S, Fasshauer M (2013) Adipocyte fatty acid binding protein: a novel adipokine involved in the pathogenesis of metabolic and vascular disease? Diabetologia 56(1):10–21. https://doi.org/10.1007/s00125-012-2737-4
Liu H, Guo M, Jiang F-L (2018) Serum concentrations of fatty acid-binding protein 4 in Chinese children with type 1 diabetes mellitus. J Diabetes Complicat 32(5):488–491. https://doi.org/10.1016/j.jdiacomp.2017.12.009
Furuhashi M (2019) Fatty acid-binding protein 4 in cardiovascular and metabolic diseases. J Atheroscler Thromb 26(3):216–232. https://doi.org/10.5551/jat.48710
Wotherspoon AC, Young IS, McCance DR et al (2016) Serum fatty acid binding protein 4 (FABP4) predicts pre-eclampsia in women with type 1 diabetes. Diabetes Care 39(10):1827–1829. https://doi.org/10.2337/dc16-0803
Patterson CC, Dahlquist GG, Gyürüs E, Green A, Soltész G (2009) Incidence trends for childhood type 1 diabetes in Europe during 1989-2003 and predicted new cases 2005-20: a multicentre prospective registration study. Lancet 373(9680):2027–2033. https://doi.org/10.1016/S0140-6736(09)60568-7
Dabelea D, Mayer-Davis EJ, Saydah S et al (2014) Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA 311(17):1778. https://doi.org/10.1001/jama.2014.3201
Große J, Hornstein H, Manuwald U, Kugler J, Glauche I, Rothe U (2018) Incidence of diabetic ketoacidosis of new-onset type 1 diabetes in children and adolescents in different countries correlates with human development index (HDI): an updated systematic review, Meta-analysis, and Meta-regression. Horm Metab Res 50(03):209–222. https://doi.org/10.1055/s-0044-102090
Usher-Smith JA, Thompson M, Ercole A, Walter FM (2012) Variation between countries in the frequency of diabetic ketoacidosis at first presentation of type 1 diabetes in children: a systematic review. Diabetologia 55(11):2878–2894. https://doi.org/10.1007/s00125-012-2690-2
Scibilia J, Finegold D, Dorman J, Becker D, Drash A (1986) Why do children with diabetes die? Acta Endocrinol Suppl (Copenh) 279:326–333
Secrest AM, Becker DJ, Kelsey SF, Laporte RE, Orchard TJ (2010) Cause-specific mortality trends in a large population-based cohort with long-standing childhood-onset type 1 diabetes. Diabetes 59(12):3216–3222. https://doi.org/10.2337/db10-0862
Wolfsdorf J, Glaser N, Sperling MA (2006) Diabetic ketoacidosis in infants, children, and adolescents: a consensus statement from the American Diabetes Association. Diabetes Care 29(5):1150–1159. https://doi.org/10.2337/diacare.2951150
Goldstein A, Haelyon U, Krolik E, Sack J (2001) Comparison of body weight and height of Israeli schoolchildren with the Tanner and Centers for Disease Control and Prevention growth charts. Pediatrics 108(6):E108. https://doi.org/10.1542/peds.108.6.e108
Wu KK, Huan Y (2008) Streptozotocin-Induced Diabetic Models in Mice and Rats. In: Current Protocols in Pharmacology. John Wiley & Sons, Inc., Hoboken, NJ, USA, p Unit 5.47
Xu A, Wang Y, Xu JY et al (2006) Adipocyte fatty acid-binding protein is a plasma biomarker closely associated with obesity and metabolic syndrome. Clin Chem 52(3):405–413. https://doi.org/10.1373/clinchem.2005.062463
Aeberli I, Beljean N, Lehmann R, l’Allemand D, Spinas GA, Zimmermann MB (2008) The increase of fatty acid-binding protein aP2 in overweight and obese children: interactions with dietary fat and impact on measures of subclinical inflammation. Int J Obes 32(10):1513–1520. https://doi.org/10.1038/ijo.2008.128
Tirosh A, Calay ES, Tuncman G et al (2019) The short-chain fatty acid propionate increases glucagon and FABP4 production, impairing insulin action in mice and humans. Sci Transl Med 11(489):eaav0120. https://doi.org/10.1126/scitranslmed.aav0120
Coe NR, Simpson MA, Bernlohr DA (1999) Targeted disruption of the adipocyte lipid-binding protein (aP2 protein) gene impairs fat cell lipolysis and increases cellular fatty acid levels. J Lipid Res 40(5):967–972. https://doi.org/10.1016/S0022-2275(20)32133-7
Scheja L, Makowski L, Uysal KT et al (1999) Altered insulin secretion associated with reduced lipolytic efficiency in aP2−/− mice. Diabetes 48(10):1987–1994. https://doi.org/10.2337/DIABETES.48.10.1987
Grabacka M, Pierzchalska M, Dean M, Reiss K (2016) Regulation of ketone body metabolism and the role of PPARα. Int J Mol Sci 17(12):2093–2116. https://doi.org/10.3390/IJMS17122093
Furuhashi M, Fucho R, Görgün CZ, Tuncman G, Cao H, Hotamisligil GS (2008) Adipocyte/macrophage fatty acid-binding proteins contribute to metabolic deterioration through actions in both macrophages and adipocytes in mice. J Clin Invest 118(7):2640–2650. https://doi.org/10.1172/JCI34750
Laffel L (1999) Ketone bodies: a review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab Res Rev 15(6):412–426. https://doi.org/10.1002/(sici)1520-7560(199911/12)15:6<412::aid-dmrr72>3.0.co;2-8
Gruber N, Reichman B, Lerner-Geva L, Pinhas-Hamiel O (2015) Increased risk of severe diabetic ketoacidosis among Jewish ultra-orthodox children. Acta Diabetol 52(2):365–371. https://doi.org/10.1007/s00592-014-0653-4
Vicinanza A, Messaaoui A, Tenoutasse S, Dorchy H (2019) Diabetic ketoacidosis in children newly diagnosed with type 1 diabetes mellitus: role of demographic, clinical, and biochemical features along with genetic and immunological markers as risk factors. A 20-year experience in a tertiary Belgian center. Pediatr Diabetes 20(5):pedi.12864. https://doi.org/10.1111/pedi.12864
Kelsey MM, Zeitler PS (2016) Insulin resistance of puberty. Curr Diab Rep 16(7):64. https://doi.org/10.1007/s11892-016-0751-5
Acknowledgements
We would like to thank N. Oz (the Dalia and David Arabov Diabetes Research Center, Division of Endocrinology, Diabetes and Metabolism, Sheba Medical Center, Tel-Hashomer, Israel) for his technical help with animal experiments. Some of the data were presented as an abstract at the 58th European Society for Pediatric Endocrinology meeting in 2019.
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Funding
A grant from the Israeli Diabetes Association supported this study (to ArT). This work was also supported in part by the Israel Science Foundation to ArT (grant no. 922/17).
Author information
Authors and Affiliations
Contributions
NG, MR, RL and SS researched the data. NG, OP-H and ArT made a substantial contribution to the design of the work and analysis and interpretation of the data. NG made a substantial contribution to collection of data in the human study. NG wrote the first draft and was responsible for all the drafts of this work including the final version. MR and RL performed the animal studies and reviewed the manuscript. MR, RL and SS provided critical comments and approved the final version to be published. SS participated in the analysis of the data EB, IR and RH participated in the laboratory analyses of the human study. EB, IR, RH, AtT and OPH took part in the critical revising of all the drafts including the final version. AtT and OP-H participated in the study design and statistical analysis of the data. ArT was responsible for obtaining all necessary resources for the study and critically revised all drafts of the manuscript, including the final version. NG and ArT are guarantors of this work. All authors approved the final version.
Corresponding authors
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(PDF 47 kb)
Rights and permissions
About this article

Cite this article
Gruber, N., Rathaus, M., Ron, I. et al. Fatty acid-binding protein 4: a key regulator of ketoacidosis in new-onset type 1 diabetes. Diabetologia 65, 366–374 (2022). https://doi.org/10.1007/s00125-021-05606-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-021-05606-0